





Abstract
Human immunodeficiency virus (HIV) is well known to be associated with various neoplasms and opportunistic infections. Kaposi sarcoma (KS), associated with human herpes virus 8 (HHV8) infection, is the most common tumour in HIV positive patients and is also an acquired immune deficiency syndrome (AIDS) defining illness. Cutaneous manifestations are the most common presenting symptom; however, visceral involvement is also recognized. We present the case of a 55-year-old male who was diagnosed with AIDS-related KS, who was referred to our surgical unit with an indeterminate left adrenal lesion. He subsequently started antiretroviral therapy and given the indeterminate nature of his adrenal lesion, we performed a laparoscopic left adrenalectomy, with KS of the adrenal gland confirmed on histology
INTRODUCTION
Kaposi sarcoma (KS) is the most common neoplasm among patients with human immunodeficiency virus (HIV) [1]. It is defined as an angioproliferative disorder which requires infection with human herpes virus 8 (HHV8) for its development [2]. Four types of KS have been classically described: classic, endemic, iatrogenic and acquired immune deficiency syndrome (AIDS)-associated. The most common, initial presentation of KS is cutaneous disease, however, visceral involvement has been observed in several sites including lung, oral cavity, gastrointestinal tract, pancreas, heart, bone and muscle [3, 4].
AIDS-associated KS of the adrenal gland is rare with few case reports in the published literature [5, 6]. As such, the investigation and subsequent management of an adrenal mass in the HIV positive patient is less clear.
We present a 54-year-old man who was recently diagnosed with HIV with cutaneous signs and symptoms diagnostic for KS. Imaging revealed probable visceral involvement of his lungs and an indeterminate lesion in his left adrenal. Laparoscopic adrenalectomy was performed and histology confirmed the presence of KS involving the adrenal gland.
CASE REPORT
A 54-year-old man was referred by his GP to the infection disease unit at his local hospital with scalp folliculitis. At that point, he also complained of a purple-bluish discolouration on the arch of his right foot. A biopsy of this lesion confirmed KS. He also had oral candida and lesions in his oral cavity suggestive of KS. HIV positive status was subsequently confirmed. His CD4 count was 144 cells/mm3 and viral load was >500 000 copies/ml and in the presence of KS, he was diagnosed with AIDS.
He was started on highly active antiretroviral therapy, pneumocystis carinii pneumonia (PCP) prophylaxis and antifungals. He had a CT scan of his chest which showed changes suggestive of sarcomatous disease in his lungs or possibly infection.
He was referred to oncology for consideration of systemic therapy for KS. Given, the stability of his disease and the significant improvement in his viral load and CD4 count, there was no clear indication for systemic therapy. A follow up CT—chest/abdomen a few months later revealed an incidental 12 × 10 mm2 enhancing left adrenal mass but no remission of his chest disease. A dedicated CT-adrenal was performed which reported an enhancing lesion with 44% washout making an adenoma less likely. Hormonal investigations to determine the functional nature of this lesion were all normal.
A whole body NM FDG PET-CT was performed. This reported high metabolic activity in his left adrenal gland with an increase in size—highly suspicious for a malignancy (Fig. 1). He was referred to the endocrine surgeons for consideration of excision of his adrenal mass and also to the thoracic surgeons for a lung wedge biopsy which confirmed KS. We performed a laparoscopic left adrenalectomy following his wedge biopsy. Intra-operatively, the adrenal gland was mobilized from adjacent structures without difficulty and there no evidence of local invasion or peritoneal disease. He was discharged the following day and had an unremarkable recovery.
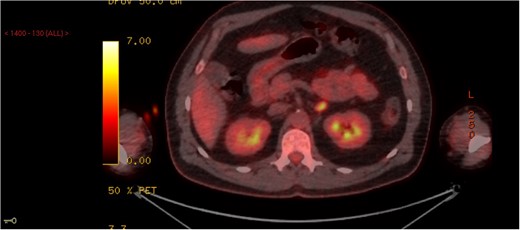
PET scan demonstrating a left adrenal lesion with high metabolic activity.
The adrenal gland parenchyma was partly replaced by poorly circumscribed tumour composed of spindle cells showing mild nuclear pleomorphism. These spindle cells were positive for CD34, CD31 and HHV8 supportive of a diagnosis of KS.
DISCUSSION
We present the case of a 54-year-old male with newly diagnosed HIV with histologically confirmed KS of the adrenal gland. While KS is common in the HIV positive patient, this is a rare case of KS involving the adrenal gland
KS is a vascular tumour associated with HHV8 infection and is the most common tumour affecting HIV positive patients [1, 2]. It is more common in homosexual and bisexual men compared to heterosexual injection drug users, women and children [1]. CD4 count is also an important risk factor for development of KS with counts of <200 cells/mm3 increasing the risk ratio compared to those with counts >500 cells/mm3 [7].
Cutaneous manifestations are often the most common and initial presentations of KS often involving the lower extremities, face and genitalia with the diagnosis confirmed by clinical exam and biopsy [6]. Visceral disease can occur at any site but the oral cavity, gastrointestinal and the respiratory tract are most commonly affected [3, 4].
Adrenal gland involvement is exceedingly rare and is an unusual location for KS [6]. Most adrenal gland lesions are picked up incidentally following imaging studies for other pathology with the reported prevalence of 4% in patients undergoing CT for other investigations [8]. The majority of these lesions are benign and non-functioning with metastases accounting for <2% of all tumours [9, 10].
The functional status of the lesion should be determined by means of urinary and plasma metanephrines, low dose dexamethasone suppression tests and 24 h urinary cortisol, plasma aldosterone concentration and plasma rennin activity.
Imaging is useful in the evaluation of an adrenal incidentaloma. CT scan is the imaging modality of choice for investigation of adrenal lesions. Change in size and characteristics of lesions are useful measures that can guide management [11].
Benign lesions appear round and homogenous with sharp margins. They also have low attenuation values (<10 HU) with rapid contrast washout >60%. Malignant lesions and metastatic disease have increase attenuation on non-enhanced CT (>20 HU) as well as delayed washout [11]. They appear irregular in shape and have an inhomogenous nature. For indeterminate lesions, PET-CT is useful if a history of malignancy exists or is highly suspected.
For patients with an indeterminate or suspicious lesion on imaging, adrenalectomy should be performed. Given the indeterminate nature of the adrenal lesion in our patient and high metabolic activity on PET-CT, it was important to exclude an adrenocortical carcinoma.
In summary, the findings of KS affecting the adrenal gland are rare. The management of the adrenal lesion should follow the same algorithm as for those patients without HIV disease.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}