





Abstract
Adrenohepatic fusion is a relatively common condition that has been reported in the literature and explained as a result of normal aging. However, the presence of a neoplastic process in the adrenohepatic fusion is relatively uncommon. A 48-year-old male presented with RUQ abdominal pain with findings of a huge liver mass with adrenohepatic fusion in the computed tomography scan. Histopathological studies revealed a mixed, although distinctly separated, adrenocortical carcinoma and a hepatocellular carcinoma within an adrenoheaptic fusion.
INTRODUCTION
Adrenohepatic fusion is a relatively common condition that has been reported in the literature and explained as a result of normal aging. However, the presence of a neoplastic process in the adrenohepatic fusion is relatively uncommon, especially when it is a malignant neoplasm. Here, we present a patient with a malignant mass consisting of an adrenocortical carcinoma and hepatocellular carcinoma arising from an adrenohepatic union.
CASE REPORT
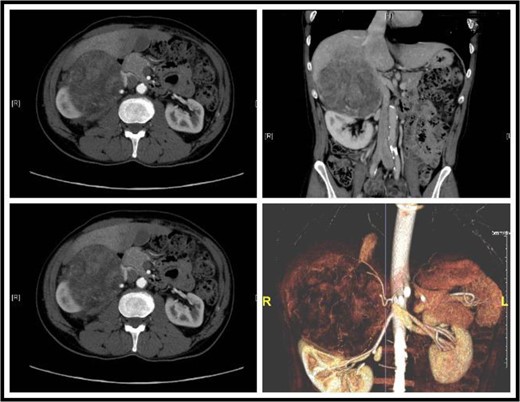
Sections of the CT showing a large retroperitoneal mass, focal absence of fat gland and an invasion into the liver.
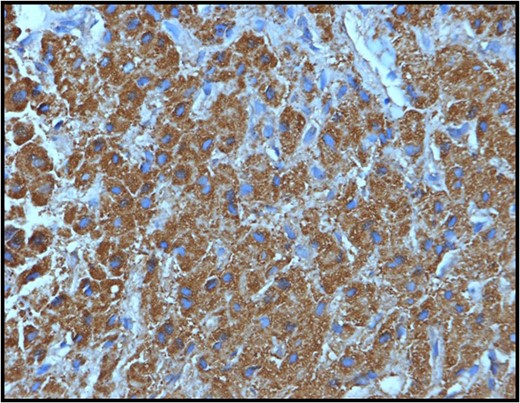
Section from the hepatic mass showing positive staining of the tumor cells with the hepar IHC stain confirming the hepatic nature of the liver mass.
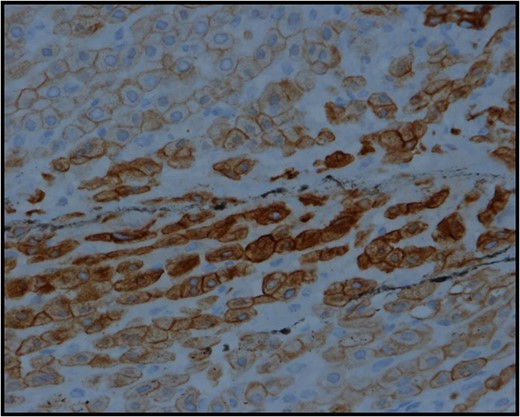
Section from the adrenocortical mass showing strong positive cytoplasmic staining with low molecular weight cytokeratin-cam 5.2 IHC stain.
DISCUSSION
Adrenohepatic fusion is a relatively common observation during autopsies [1]; however, neoplasms arising from the union are very poorly reported. In our case, an adrenohepatic fusion was detected using a CT scan of the abdomen that showed focal areas of loss of fat gland between the retroperitoneal mass and the liver. Dolan defined adrenohepatic union as the adhesion of the liver and the right adrenal cortex with the partial or complete absence of a fibrous capsule dividing the two organs [2]. Adrenocortical adenoma arising from an adrenohepatic union was reported in several cases [3]; however, we could not find a report that describes an adrenocortical carcinoma combined with a HCC from an adrenohepatic union in the literature as the case we present here. A differential diagnosis of HCC must be considered in such a case as the histopathology of the resected lesion shows mixed malignancies of adrenocortical carcinoma in the adrenal part of the lesion and a HCC in the hepatic part and several cases were reported in the literature of a primary HCC extending into the right adrenal directly [4], or to both adrenals as the first presentation of HCC metastasis [5], other reports mentioned cases where an HCC has developed in an ectopic liver tissue [6]. On the other hand, an adrenocortical tumor that developed from an adrenal rest inside the liver with radiological findings of HCC was also reported [7]. Okuda introduced a few cases of HCC presenting as pedunculated masses outside the liver most of which had dual blood supply of a hepatic and a suprarenal artery that might support the fusion phenomenon, furthermore, none of the masses were discovered in the left adrenal, which, again, supports fusion and invasion rather than hematogenous spread [8]. Core biopsy was reported in different similar cases to be of diagnostic value that changed the presumed diagnosis based solely on imaging modalities [5]. In our case, after using a CT scan to diagnose the patient, a trucut biopsy was done to confirm the diagnosis of an adrenocortical carcinoma invading the liver; however, an incidental histopathologic finding of co-occurrence of a HCC in the same lesion raised our suspicions, so we went to do a positron emission tomography scan CAP to look for any focus of metastasis, which revealed negative results. Surgical resection is the gold standard option to manage both HCC and adrenocortical carcinoma [5]. The patient was followed up for 2 years after the operation without evidence of metastasis or recurrence.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}