





Abstract
A mesenteric cyst is rare intra-abdominal pathology, with little literature to guide us on how to diagnose and manage it. We report the incident of a 57-year-old female who had an incidental finding of a sigmoid mesenteric cyst whilst undergoing an operation under the care of the Gynaecologists. A computed tomography scan and a flexible sigmoidoscopy followed to help diagnose the lesion as a cyst. A month later the 10 × 15 cm2 cyst was excised laparoscopically with no complications.
INTRODUCTION
Mesenteric cysts are rare intra-abdominal lesions [1–4]. They occur in both adults and children with an incidence of 1/10 500–25 000 of adult surgical patients [5]. They are mostly found incidentally but patients with these cysts can sometimes present with non-specific complaints of abdominal pain and distension, or an abdominal mass [1]. They commonly originate in the small bowel mesentery, mesocolon (24%), retroperitoneum (14.5%) and very rarely from the sigmoid mesentery [6]. To diagnose these cysts, patients often require radiological investigations such as ultrasonography (USS), computed tomography (CT) and magnetic resonance imaging (MRI) [7]. Depending on their symptoms and location, these cysts can either be treated conservatively, or by open or laparoscopic surgical excision, and histological examination is often required to identify the origin of the cyst.
CASE REPORT
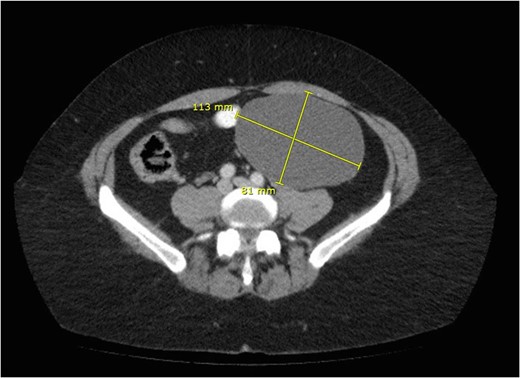
CT scan showing cyst.

Coronal plane of CT.
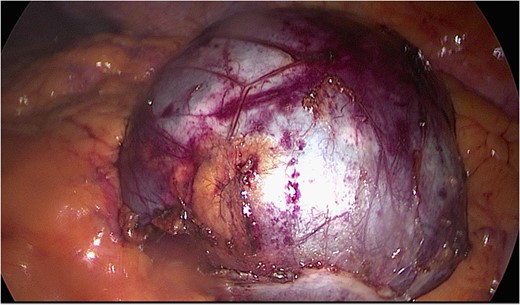
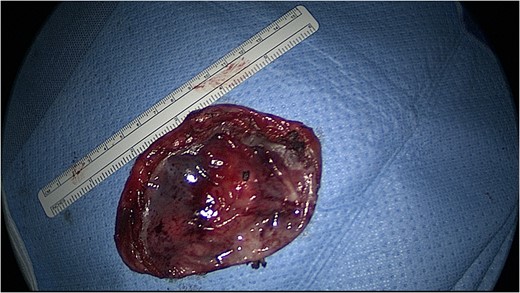
Image of sigmoid mesenteric cyst.
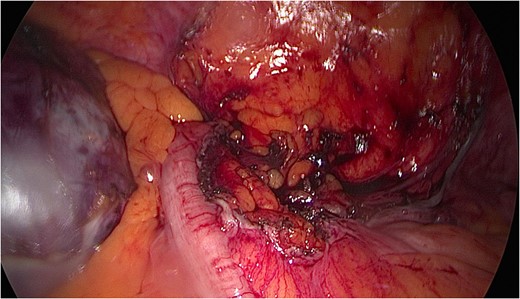
Sigmoid mesentery with cyst excised.
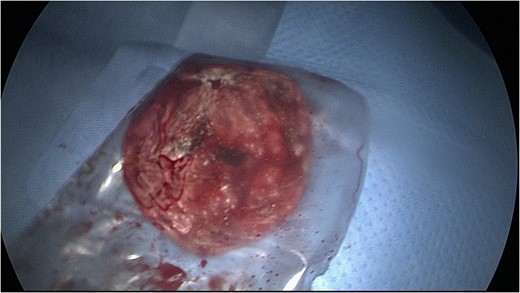
Cyst drained and removed using an endocatch.
Cyst drained measuring about 11 cm.
The rest of the abdominal cavity was washed with normal saline and closed. Since, the patient has made a full recovery and is completely symptom free. The histology report suggests the mass to be a borderline mucinous cystadenoma with either ovarian or appendiceal origin.
DISCUSSION
Little information is available in the literature on how to manage patients with symptomatic mesenteric cysts. In addition to being a rare entity, these cysts can pose a diagnostic challenge because patients often present with non-specific symptoms and an excision biopsy is often required to ascertain the origin of the cyst. In the case we describe here, the patient presented with left iliac fossa pain and swelling for 10 month, which are similar to the symptoms mentioned by Bhandarwar et al. [1]. Other possible symptoms can be suprapubic abdominal pain and back ache for 2 months [7] or 4 days duration of generalised abdominal pain that had moved to the RIF associated with diarrhoea and vomiting [8].
Investigations for sigmoid mesenteric cysts have previously included USS and CT [1, 7]; while in one case the symptoms were so severe that no radiological investigations were performed and the patient was taken to theatre for laparotomy for suspected appendicitis [8].
The approach to managing mesenteric cysts vary in the literature. In the acute setting papers have suggested that laparotomy should be the method of choice [8] but more recently there has been a shift to favour a laparoscopic approach [1]. Various laparoscopic techniques have been reported, however, the optimal approach for the best outcome is still unknown due to the rarity of the condition.
Although these cysts are found in the sigmoid mesentery, they can have communication with other organs that they may have originated from in the first place [6]. In the case we described we found on histological examination that the cyst was a cystademona. In the reports that we found during our literature review the histological findings were a benign mucinous mesenteric cyst [7] and a benign lymphangioma [1] and a mesenteric cyst with a thin fibrous wall, showing early and mild acute inflammation [8].
CONCLUSION
The paucity of literature on mesenteric cysts makes it difficult to create a gold standard for the management of these patients, however, in other most similar cases there has been a thorough step-wise approach. Most patients are managed electively with an investigation in the form or an USS or CT scan to establish the characteristics of the mass and its involvement of surrounding structures. Where possible a laparoscopic approach is favourable. Various laparoscopic techniques have been reported, however, the optimal approach for the best outcome is still unknown due to the rarity of the condition.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}