





Abstract
Complete mesocolic excision (CME) is a standardized surgical procedure for colonic cancer that requires ample knowledge of the anatomical patterns of the colic arteries. Variations of the colic vessels encumber both surgical and endovascular techniques. In the presented case below, the right colic artery was incidentally detected emerging from the right gastroepiploic artery, during CME. Surgeons should be always aware of this variation in order to perform safe abdominal surgeries and sufficient resection of the regional lymph nodes with a view to minimizing the probability of recurrence of disease when encountering colonic cancer.
INTRODUCTION
Complete mesocolic excision (CME) is a standardized surgical procedure for colonic cancer [1]. When performing CME, the origin of the colic arteries has to be adequately exposed and tied centrally to ensure maximal possible dissection of the regional lymph nodes. This surgical step is of great importance, since it certifies better therapeutic outcomes and survival [1, 2]. Nevertheless, the colic arteries may present multiple anatomic variations which encumber the operation [3]. In the presented case, the right colic artery (RCA) was incidentally detected emerging from the right gastroepiploic artery, during CME. To the best of our knowledge, this is the first reported case of such an anomalous origin of the RCA in the literature.
CASE REPORT
A 67-year-old female patient proceeded to our institution with a 2-month history of intense fatigue and vague abdominal pain in the right lower quadrant of the abdomen which progressively became worse. The patient had no previous surgical history. Clinical examination was unremarkable without any positive signs, tenderness or any palpable masses. Blood tests revealed anemia (Ht: 35% and Hb: 10 mg/dl). An abdominal CT scan detected malignant lesions of the ascending colon. Subsequent CT scan of the chest had no evidence of metastasis. A colonoscopy confirmed the CT scan findings. Following these, CME was scheduled.
During the operation, surgeons attained to isolate the main supplying arteries of the right colon and their origins. The ileocolic and the middle colic arteries were observed, as typically, emerging as isolated vessels from the superior mesenteric artery (SMA). However, the origin of the RCA was nor observed from the SMA, nor from the previous arterial branches, as in common. Surgeons continued ascending dissection in order to detect the origin of the RCA that was finally observed arising from the right gastroepiploic artery (Figs 1–2). Pericolic lymph nodes and the lymph nodes that followed the central wards of the ileocolic, the middle colic and the aberrant RCA were gently dissected. The operation continued in the usual pattern. A drainage was placed and was finally removed the 6th postoperative day. The patient was discharged the 10th postoperative day with instructions. At the follow-up, the 14th postoperative day, the patient suffered no complications whatsoever.
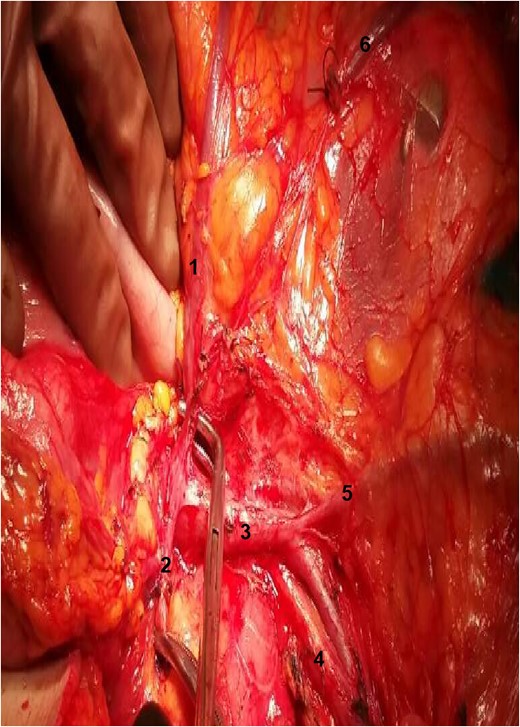
Exposure of the operative field. 1: RCA; 2: gastroepiploic artery; 3: superior mesenteric vein; 4: SMA; 5: ileocolic vein; 6: stump of right colic vein.
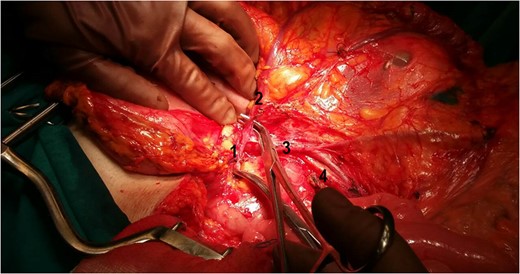
The relation between the vessels: 1: gastroepiploic artery; 2: RCA; 3: superior mesenteric vein; 4: SMA.
DISCUSSION
The surgical technique of CME for colonic cancer is closely related to lower local recurrence of the disease and better survival [1]. The extent of the procedure is determined by the location of the malignant lesion and the pattern of the lymphatic spread. For malignancies of the right colon, as in the presented case, identification of the origins of the ileocolic, the middle colic and the RCA is essential for ample lymph node dissection [4]. It is well established though in the literature, that the colic arteries may present a lot of anatomical variations [3]. Indeed, it is considered that the RCA is the responsible anatomic structure for major variations [3].
The RCA supplies the main part of the ascending colon till the hepatic flexure and typically originates as an isolated branch from the SMA [5]. Nevertheless, there are several variations documented in the literature. In fact, RCA may emerge from a common trunk with the middle colic or the ileocolic artery respectively. In addition, all these arteries may arise simultaneously from a common arterial branch of the SMA [3]. The absence of the RCA has been described in the literature as well [3, 6, 7]. Finally, another interesting variation of the RCA was its direct origin from the abdominal aorta [8]. Apart from the meticulous review of the existing literature and anatomy textbooks, anomalous origin of the RCA from the right gastroepiploic artery, as in the presented case, could not be found.
The etiology of such a variation of the RCA remains vague, but as it is believed, formation of similar anatomical variations may be through anastomoses between the arterial branches of the diffuse capillary plexus [7, 8].
Furthermore, variations of the RCA are of key clinical significance since encumbering abdominal surgical and endovascular procedures [8]. Thus, such aberrant vessels may be incidentally injured during such processes and lead to severe bleeding and colic ischemia. Additionally, such variations of the RCA are related to the therapeutic outcomes of CME and other colonic cancer surgical treatments. More specifically, failing to identify the anomalous origin of the RCA may result in suboptimal lymph node harvest. Finally, such variations of the RCA should be also considered when performing angiography in order to detect the source of gastrointestinal bleeding [8].
In conclusion, anomalous origin of the RCA of the right gastroepiploic artery consists a unique anatomic variation of major clinical significance. Hence, surgeons’ thorough knowledge concerning the variability of the RCA, in addition to perpetual awareness and detailed exposure of the operative field during the operation, are the cornerstone of a safe abdominal surgery and optimal lymph node dissection in case of colonic malignancy.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}