





Abstract
Scrotal pain presentation has many differential diagnoses such as testicular torsion is surgical emergency. For this reason, it is necessary for surgeons to differentiate between diseases for choosing the best treatment approach. We have reported a rare condition of 19-year-old male case had an atypical scrotal pain presentation of appendicitis. He was admitted to emergency service with 4 days history of pain in abdomen and testis. In physical examination, there is tenderness in right lower quadrant, right inguinal region and scrotum. Testicular torsion and appendicitis were roll-out in sonography. Because of low sensitivity of sonography in diagnose of appendicitis and high suspicious of surgeons, the case was candidate for an open appendectomy surgery. Acute suppurative appendicitis that presenting testicular pain is rare for making the best diagnosis and prevents multiple surgeries in such cases, cooperation of urology, general surgery and radiology specialists with high index of suspicion is required
INTRODUCTION
Pain presentation in scrotum revealed many differential diagnoses in adult patients such as testicular torsion and infections. The best diagnosis for roll-out of such diseases is history and physical examination and for confirming of probable diagnosis using lab tests and color-Doppler ultrasonography is recommended. There have seen few cases of an atypical scrotal pain presentation. This study reports a case with suppurative appendicitis lead to an atypical scrotal pain presentation.
CASE PRESENTATION
A 19-year-old male was admitted to the emergency service complaining of pain in abdomen and testis. The pain began 4 days prior. Also, the patient complains of nausea and vomiting, fever and chills and loss of appetite without symptoms of urinary problems. He had habit of smoking but nothing about previous diseases and taking medications in his history. No history of trauma was mentioned. Physical examination revealed an ill man with following vital signs: blood pressure 120/80 mmHg, respiratory rate 18 breaths per minute, and temperature 39.5°C, pulse rate 100 beats per minute. Tenderness was appreciated in right lower quadrant (RLQ), right inguinal region and scrotum with radiating to the right groin area. Abdomen was soft, symmetric and no signs of distention, guarding, with positive rebound tenderness and Rovsing’s sign. Significant laboratory results included white blood cell count = 16.5 × 103/mic L (normal range 4.4–11.0), hematocrit = 40% (normal range 41.5–50.4), Sodium = 131 mEq/L (normal range 138–145), platelet distribution width = 10.1% (normal range 12.0–20.0) and the other laboratory tests such as: R.B.C Count, Hemoglobin, MCV, MCH, MCHC, Platelet, Lymphocytes count, Fasting Blood sugar, BUN, creatinine and urine analysis (U/A) were normal. Abdominal and pelvic ultrasonography revealed features in enlarged lymph node and free abdominal fluid in RLQ. Any significant inflammation, abscess and mass in appendix were not reported. Also, the radiologist recommended consideration of other clinical and paraclinical signs and symptoms to rule out appendicitis. In according to the order of urologist sonographic color-Doppler requested and no significant abnormal findings were reported. Hence, general surgeon decided to perform appendectomy at Mcburney’s point. As the report of surgeon appendix was suppurative. Also, surgeon observed 100 cm of ileum for any additional problems (Figs 1 and 2).
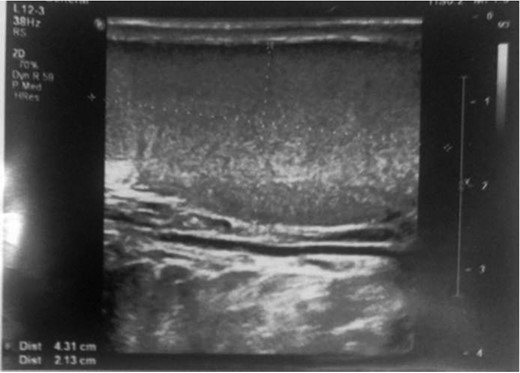
Ultrasound picture of the testis showed normal echogenicity without any abnormality.
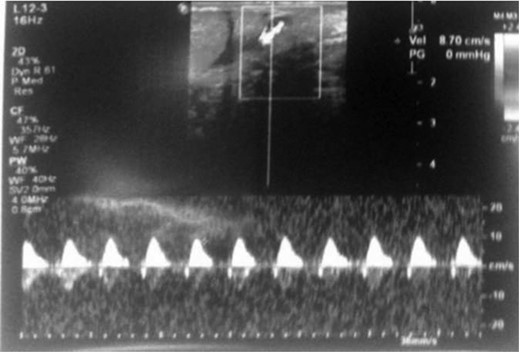
Doppler ultrasound using gray scale method of the testis showed normal flow pattern of testicular artery.
DISCUSSION
In acute scrotal pain, testicular and appendicular torsion must be considered as a urological emergency. Also, Infections such as epididymitis and epididymo-orchitis should be rolling out by physical examination and Doppler ultrasonography. Suppurative appendicitis with scrotal pain is very rare. Many similar cases have reported in recent years with the appendicitis and findings are confounded by testicular torsion of appendix. In this case a 14-year-old boy with lower abdominal pain and right testis tenderness and swelling but there were not any sign of rebound and guarding. Surgeons have reported Suppurative appendicitis with an open processus vaginalis in the surgery. This can make a track that pus down an open processus vaginalis [1].
There are many types of atypical presentations for appendicitis such as hyper-amylasia and testicular pain mimicking pancreatitis or testicular torsion presentations. In Durai et al. study [2], Renu kumar et al. reported a 26-day-old patient pain of representing testicular torsion with associated UDT that finally diagnosed with appendicitis by using of nuclear scintigraphy [3]. indeed, perforated appendix may lead to intra-abdominal abscess that may extend to pelvic and presenting scrotal pain [4].
Also, there are many studies which has reported acute appendicitis represented with epididymo-orchitis for example in Suppiah et al. study, reported a 61-year-old man who presented a right testicular pain, scrotal erythema and increasing in markers of inflammation (CRP and leukocytes were increased). The CT scan showed inflammation of appendix within small direct type of inguinal hernia [5].
Acute epididymitis in patients with pain in groin should roll-out by using lab tests of CDC guidelines includes: more than two WBC per oil immersion field in gram stain of urethral secretion, leukocyte esterase on first voiding should be positive and more than 10 WBC per high power field in sedimentation of first voiding microscopic examination [6] also, color-Doppler ultrasonography shows increases in blood flow of epididymis for diagnosing of epididymitis
To make the best diagnosis and prevent multiple surgeries in such cases, cooperation of urology, radiology and general surgery specialists with a high index of suspicion is required.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}