





Abstract
Down-sloped or hooked acromion morphologies may cause bony encroachment on the soft tissues of the subacromial space, predisposing to shoulder impingement syndrome. Of the latter, a hooked or Type III acromion (T3A) has also been linked to rotator cuff (RC) pathology. However, as bony acromial impingement is typically thought to occur over the age of 40, its occurrence in younger shoulder athletes presenting with shoulder pain, impingement and RC pathology may be overlooked. This case serves to illustrate the occurrence of T3A in a younger shoulder athlete, and the importance of early imaging in achieving diagnostic accuracy. Appropriate surgical referrals are patients with subacromial impingement syndrome refractory to 3–6 months of appropriate conservative treatment. Surgery may be particularly beneficial in patients with a T3A.
INTRODUCTION
Although typically thought to occur in older individuals, a hooked acromion causing shoulder impingement symptoms in younger populations is less recognized. Early identification of bony impingement may prevent unsatisfactory treatments and guide more effective management.
This report illustrates a case of Type III acromial impingement in a younger athlete and the importance of early imaging in refining diagnosis.
CASE REPORT
A 31-year-old right-hand dominant cross-fit personal trainer presented to an outpatient clinic complaining of left shoulder pain worsening over a 2-year period. The pain had become intermittently worse over the last 6 weeks, and was particularly flared the day following handstand push-ups and kipping. Pain was reportedly worsened by shoulder abduction beyond 90°, bicep hammer curls and eccentric bench press. The patient perceived the left shoulder to be more elevated than the right at rest, and he had begun to note joint crepitus on circumduction. The pain was focal to the anterior aspect of the deltoid and upper biceps region with an occasional pulling sensation in the distolateral biceps. The patient was perplexed as to why the left shoulder was painful when he was right-handed. He described a 3–8/10 baseline daily pain, increasing to 10/10 with bicep curls and eccentric bench press. He reported that using an elbow sleeve brace provided some temporary relief. He pain with activities of daily living such as removing his shirt, lifting his 2-year-old child, and he was unable to sleep on his left side. Despite the pain, he had never rested for more than a few days. He had, however, decreased bench press weight. He had no history of shoulder injuries. There was no reported neck pain or radiculopathy. His SPONSA score was 40% [1].
The balance of his past medical history was generally unremarkable. He took no medications, had no reported drug allergies or prior reactions to anesthesia. His family history was also unremarkable.
He was a non-smoker, and had been engaged in professional power lifting since 2008.
The patient presented with a neutral posture. Both shoulders were well muscled bilaterally without scars deformity or atrophy. On examination, cervical spine ranges of motion were pain free and the Spurling's test with extension was negative [2].
A painful arc was present upon left shoulder abduction with hitching a reported pain at 90°. There was, however, no palpable or audible crepitus on left shoulder circumduction. The patient reported that this routinely occurred but eased somewhat after warm-up. The Hawkin's test was positive. Speed's, scarf, empty can tests were negative. Elbow range of motion was full and pain free. However, there was a focal area of tenderness upon palpation 3 cm proximal to the left lateral epicondyle. Mill's & Cozen's tests were negative, and resisted muscle testing of the common extensor origin and extensor carpi radialis brevis was unremarkable. The left proximal biceps tendon and medial aspect of the left acromial-clavicular joint (ACJ) was focally tender on palpation. Thoracocervical palpation was generally unremarkable and the lift-off test was negative. The upper limbs were neurovascularly intact.
The initial diagnostic impression was of chronic left shoulder impingement (query subacromial bursal effusion, early rotator cuff (RC) tear, down-sloped acromion), and mild ACJ osteoarthritis. Although the physical examination was generally unremarkable, the history was indicative of some mild left extensor origin biceps tendonopathy.
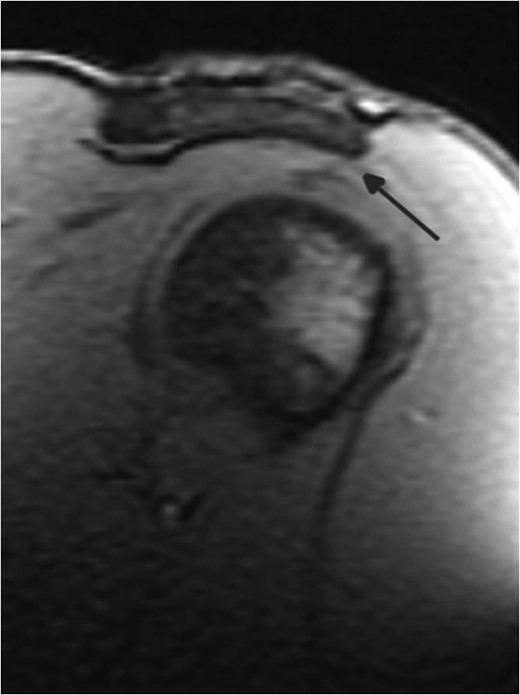
MRI shoulder.
The report of imaging findings and prognostic discussion convinced the patient of the importance to alter the intensity of his upper body training activities. By simply avoiding repetitive overhead activities and modifying the intensity of his upper body exercise program, impingement symptoms abated considerably over a period of several weeks. As the patient was responding to conservative management and there was no evidence of RC tear on imaging, surgical referral was postponed.
DISCUSSION
There are several functional and potentially reversible causes of shoulder impingement syndrome. However, identifying the presence of bony impingement of the subacromial space may aid in a better understanding of predispositions to RC pathology.
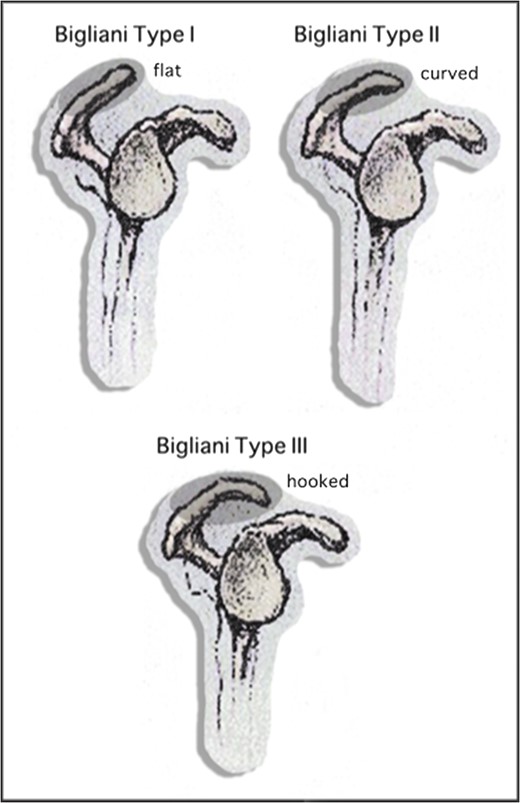
Acromial morphology.
Some studies have identified a significant association between Type III acromial morphology and full thickness RC tears [4].
Although Type III acromion (T3A) may be rare in asymptomatic young athletes, the incidence of in a general population of both young and older individuals is still not completely understood [5].
Typically, older patients are noted to have a high incidence of T2A and T3A (93% of those over 70) and both of full and partial-thickness RC tears were more commonly with these morphologies than Type I [6].
Neer concluded that 95% of RC tears are caused by mechanical impingement [7], associating RC tears with extremely hooked (>43°) anterior acromial slope. Other studies have looked at the lateral extension and angulation of the acromial slope also being important in diagnosing and managing impingement pathologies [8].
Although thought to be associated with older populations, T2 down-sloped and T3 hooked acromial impingement may occur in younger populations such as overhead athletes. Impingement may be manifested by pain with overhead activities, shoulder weakness and decreased range of motion. Early shoulder X-rays including the outlet ‘Y’ view to define acromial morphology [9], or MRI imaging may help to refine diagnosis, prevent inappropriate therapies, understand prognosis and expedite more effective management strategies.
Appropriate surgical referrals are patients with subacromial impingement syndrome refractory to 3–6 months of appropriate conservative treatment.
Surgery may be particularly beneficial in patients with a T3A [10].
ACKNOWLEDGEMENTS
The authors would like to thank Mr Ken Faulkner of Whittier California for his assistance in graphic design.

{kind=link}
{kind=link}