





Abstract
Morgagni hernia is the rarest of all congenital diaphragmatic hernias, first described in 1769. It is rarely symptomatic and found on routine radiological examinations for other conditions. Gastric outlet obstruction in adults with Morgagni Hernia is exceedingly rare. An 80-year-old man was taken to the operating room with a diagnosis of Morgagni hernia with gastric outlet obstruction. An upper midline laparotomy was performed, and the incarcerated pylorus and antrum of the stomach reduced with primary closure of the defect. Postoperative period was uneventful, and the patient was discharged on the sixth postoperative day. Morgagni hernia is exceedingly rare in adults and may present with gastric outlet obstruction in the emergency room. This clinical entity should be kept in mind while evaluating the patient, and early surgical intervention should be initiated.
Introduction
Hernia of Morgagni was first described by Giovanni Battista Morgagni, an Italian anatomist and pathologist in 1769 [1]. It is a rare cause of diaphragmatic hernia usually presenting in children [1]. The defect involves failure of fusion of the septum transversus, the diaphragm and the costal arches [2]. Even though the resulting space is often congenital, conditions such as pregnancy, trauma, chronic cough, obesity and constipation, all of which may increase intraabdominal pressure predisposes the condition [3, 4]. Usually asymptomatic patients may have symptoms such as abdominal discomfort, bloating, vomiting and bowel obstruction [1]. Morgagni hernia is an uncommon cause of gastric outlet obstruction with very few case reports in the literature.
Case Report
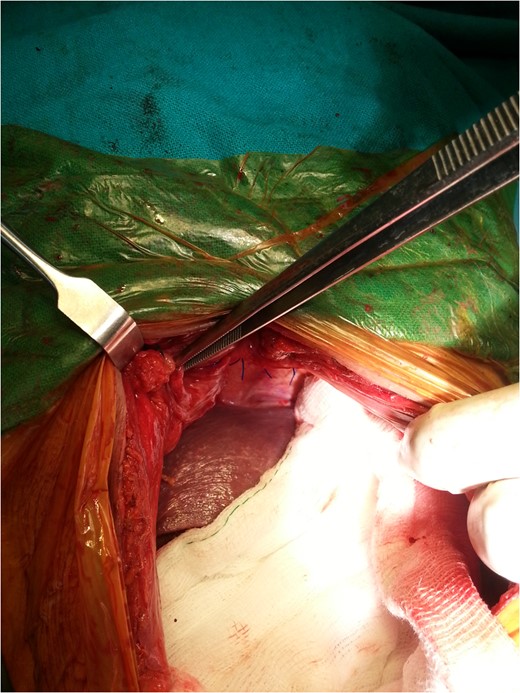
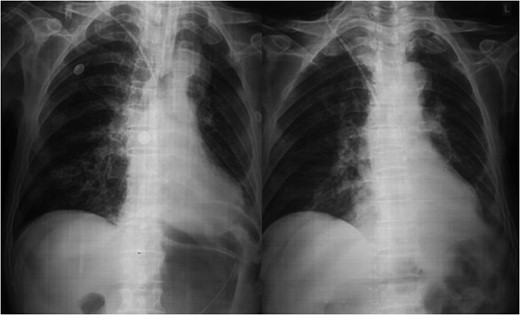
An 80-year-old man presented to our emergency room with multiple episodes of non-bilious vomiting for 4 days and not-passing stool or flatus for 2 days. He also complained of intermittent pain in the upper abdomen, which was not associated with fever, chest pain, melena or diarrhea in the recent past. However, he complained of increased cough and shortness of breath for the last 4 days on the background of a diagnosed chronic obstructive pulmonary disease. There were no similar complaints in the past. On examination, his vital parameters were normal, other than an oxygen saturation of 82% for which oxygen had to be given via face mask. His abdominal examination revealed epigastric fullness with tenderness in the epigastric and right hypochondrium. There was no evidence of peritonitis. Laboratory investigations revealed hypokalemia (3.1 mEq/l) with other parameters being normal. On the chest X-ray obtained, we saw air–fluid levels in the right thoracic cavity (Fig. 1). Computed tomography (CT) scan of the abdomen performed demonstrated a right anterior diaphragmatic hernia with stomach as content. (Figs 2 and 3) The patient was taken to the operating room, and an upper midline laparotomy was performed. Findings included an ~4 × 3 cm defect to the right of the sternum in the anterior diaphragm (Fig. 4), with incarcerated pylorus/antrum of stomach as contents and a grossly distended stomach. Rest of the bowel was normal. The contents were reduced, and the defect closed primarily with 2-0 non-absorbable interrupted mattress sutures (Fig. 5). Postoperative period was uneventful, and chest X-ray revealed a corrected defect with reduced contents (Fig. 6). The patient was started orally on the first postoperative day and discharged on the sixth postoperative day.
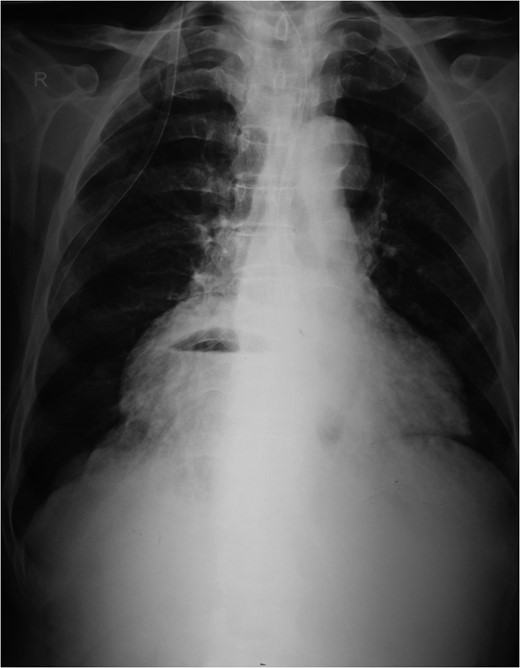
Preoperative chest X-ray.
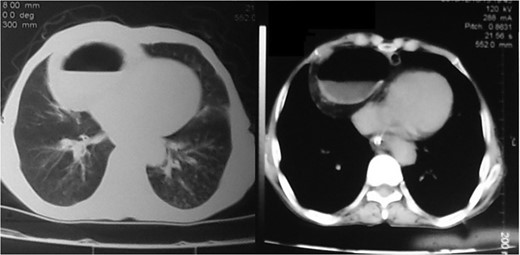
Preoperative axial CT images.
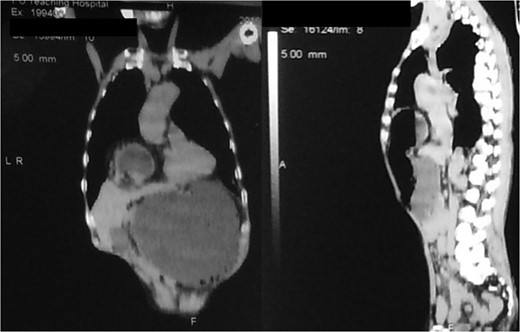
Preoperative coronal/sagittal CT images.
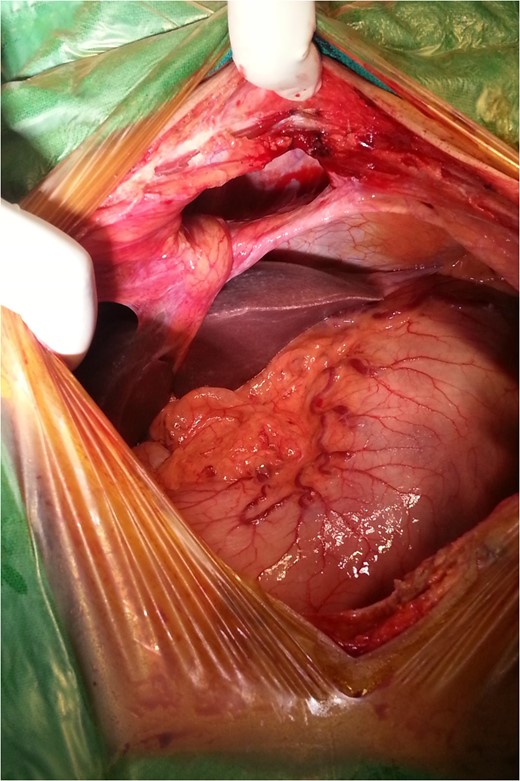
Intraoperative findings.
Post repair.
Postoperative X-ray.
Discussion
Morgagni hernia is the rarest of all congenital diaphragmatic hernias with an incidence of ~3% [3]. It occurs through the foramina of Morgagni lying between the sternal and the costal margins of the thoracic diaphragm and was first described in 1769 [1]. Although the hernias are congenital, they rarely present in children and usually are incidentally found on routine radiological imaging in adults [3]. Symptoms if present are often nonspecific, including abdominal discomfort, bloating, vomiting and bowel obstruction [1]. Emergency presentation in such patients are commonly acute respiratory distress, gastric outlet obstruction or strangulation/ischemia of entrapped bowel [5, 6], with an incidence of 12–14% [2].
Diagnosis is usually suggested by chest X-rays indicating an air–fluid level in the chest with Barium studies revealing contrast in the stomach/bowel herniating through the diaphragm. CT scan of the chest and diaphragm are highly accurate and help proceed with surgical management [7].
Surgical management via laparotomy is the most common surgical approach [3] with advantages of easier reduction of hernial contents, inspection of the contralateral diaphragm for other hernia defects and easier evaluation and surgical treatment of the acute complications, such as strangulation and ischemia of luminal abdominal organs [8]. Other techniques such as thoracotomy, thoracoscopy and laparoscopy may be used. The laparoscopic approach has the benefits of less postoperative pain and earlier return to activities and work but is less suited to emergency presentations where surgical resection or treatment of necrotic or ischemic contents may be required [3, 9].
Morgagni hernia is an exceedingly rare hernia in adults and may present with gastric outlet obstruction in the emergency room. This clinical entity should be kept in mind while evaluating the patient, and early surgical intervention should be initiated.
Ethical approval was not required from the Institute of Medicine IRB for Case Reports.
Conflict of interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}