





Abstract
When endovascular treatment is performed, angulation of the access route for a device can make the operative procedure difficult. We encountered a case in which we successfully completed thoracic endovascular aortic repair (TEVAR) in a patient with severely angulated aorta by applying ‘double-wire technique’. The patient was an 80-year-old woman. An aneurysm with a 71-mm diameter was observed in the descending aorta. We performed TEVAR. Device delivery could not be achieved by a conventional procedure using one guide wire since the peripheral aorta was severely angulated. Therefore, in addition to a guide wire for main body, a stiff wire and a stiff sheath were introduced to straighten the angulation. The device was successfully introduced and TEVAR was completed. We used the Relay Plus® that facilitates tracking through the angulation. The device has a dual structure consisting of a hard sheath and a flexible sheath. We performed TEVAR successfully.
Introduction
Thoracic endovascular repair (TEVAR) has become one of the best treatments for aortic diseases [1]. However, endovascular treatment can be difficult to perform due to challenging anatomical characteristics. Angulation of the common iliac artery or external iliac artery commonly interferes with endovascular treatment for aortic aneurysm, while aortic angulation rarely causes difficulty in performing surgery [2, 3]. We report the operative procedure for a case of severe aortic angulation in which traditional TEVAR would have been difficult.
Case Report
An 80-year-old woman with a past history of cerebral stroke and myocardial infarction was referred to our hospital for treatment of a true fusiform aneurysm (maximum short diameter, 71 mm) in the descending aorta. The preoperative contrast computed tomography (CT) images showed severe angulations in the abdominal aorta and thoracoabdominal aorta below the aneurysm. The most severe angulation was 164° in the thoracoabdominal aorta (Fig. 1). Device delivery was predicted to be challenging.
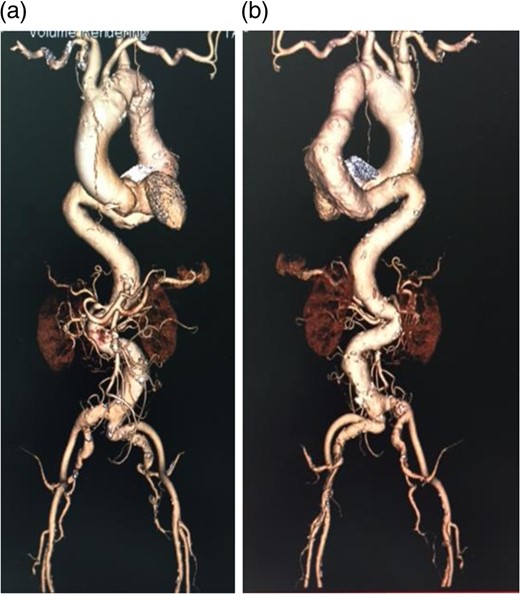
Preoperative contrast CT 3D image. (a) Anterior view, (b) Posterior view. A severe angulation was observed in the distal site of the thoracic descending aorta. Many angulations were also found in the peripheral vasculature.
We decided to perform TEVAR with the additional insertion of a stiff wire to reduce the angulation.
Operative Findings and Technique
A stiff guide wire (Amplatz Super Stiff™, 0.035 in/260 cm, Boston Scientific, Costa Rica/Heredia) was placed with its tip facing toward the ascending aorta through the right common femoral artery.
As predicted before surgery, stent graft placement was considered impossible because of the severe angulation. In an attempt to overcome this challenge, we first changed the wire to a more stiff wire (Lunderquist® Extra-Stiff Double Curved Exchange Wire Guide, 0.035 in/300 cm W Curved, Cook® MEDICAL, Denmark/Bjaeverskov), but we still could not place the stent graft.
A stiff sheath (Destination®, 6 Fr 90 cm, Terumo, Tokyo) was introduced from the left side. The sheath was placed beyond the aneurysm. Lunderquist® guide wire was introduced through the sheath. The aortic angulation was straightened and the most severe angulation below the aneurysm was reduced (Fig. 2).
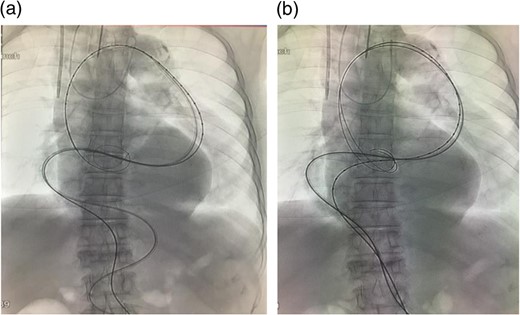
(a) A sheath was introduced and the angulation was slightly reduced. (b) A guide wire was introduced through the sheath. The angulation was further reduced by this procedure. In addition, the angulation of the wire (black arrow), which was used to introduce the stent graft main body, was reduced. Thus, the wire was advanced through the aorta where angulation was small.
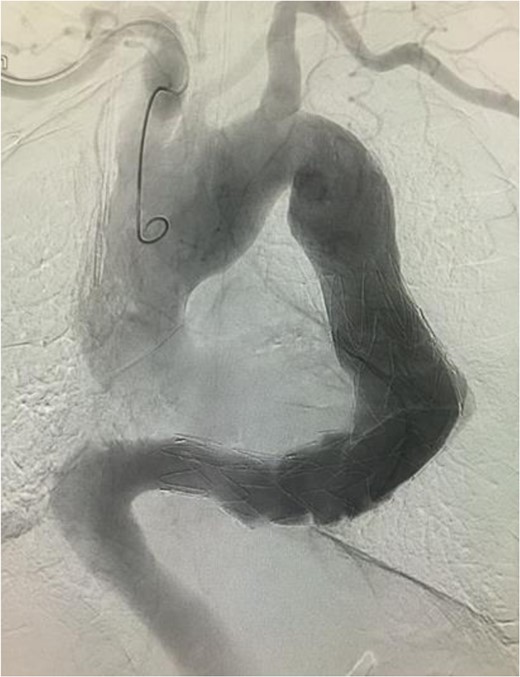
The stent graft (Relay Plus® 38 × 34 × 200 mm, Bolton medical, Barcelona) was introduced through the right common femoral artery. When it reached the distal site of the thoracoabdominal aorta where the angulation was the most severe, the outer hard sheath was left there while the inner flexible sheath was advanced. The flexible sheath was successfully introduced to the proximal site of the thoracoabdominal aorta beyond the angulation (Fig. 3). The stent graft was placed and we confirmed that no endoleak existed (Fig. 4).

Intraoperative arteriogram. (a) The hard sheath was left at the distal site of the angulated part and the flexible sheath was advanced. The angulation was sufficiently reduced by additionally introducing delivery devices for the stent graft (sheath and guide wire). Thus, the stent graft was introduced to the proximal side of the angulated part beyond the aneurysm. Compared to the preoperative contrast CT coronal section image (b) a reduction in the angulation of the proximal aneurysm was observed.
Angiographic image at the completion of treatment. No endoleak was observed. There was no contrast enhancement in the location of the aneurysm.
Postoperative Course
The patient was discharged without any complications.
Discussion
Problems can arise when endovascular treatment is performed if the vessel is severely tortuous.
Generally, angulation in the aortoiliac area is a concern. In a study on endovascular treatment for abdominal aneurysms, severe angulation in the iliac area was found in 24 of 74 cases during device delivery, and 3 cases (4%) required creating a ‘pull through’ between the angulation and the brachial artery [4]. Angulation of the aorta usually does not cause problems.
Endovascular treatment of intracranial aneurysms is likewise complicated by vessel tortuosity. If angulation of the vessel distal to the carotid artery is severe, devices cannot be introduced, often preventing the surgery from being completed [5]. To overcome this challenge, Lopes et al. reported the double-wire technique [6]. In this technique, a stiff microwire was added to reduce the vessel angulation, rendering the operation feasible. Furthermore, reports indicated that device insertion in endovascular treatment of head and neck regions was facilitated by adding a wire or microcatheter [7, 8].
In this case, TEVAR was performed for a thoracic aneurysm. The patient was at high intraoperative risk because the tortuosity and angulation of the aorta were severe. We successfully completed surgery by straightening the aortic angulation using a technique, similar to the double-wire technique.
We thought that adding one stiff wire alone would not reduce the aortic angulation sufficiently to introduce the stent graft. Thus, two methods were suggested: adding two wires or adding a stiff wire and a stiff sheath. In the latter method, a stiff sheath would be introduced to the proximal site over the aneurysm and the sheath used to straighten the angulation, then the Lunderquist guide wire would be passed through the sheath to enhance stiffness.
Using a sheath protects the aortic wall more effectively than using a wire alone, which directly contacts the aorta wall when force is applied to straighten the angulation. The use of a sheath through the angulated region and aneurysm allows the addition of more wire to facilitate vessel straightening when more force is required.
Based on the considerations above, we employed a technique in which a stiff long sheath was introduced through the left common femoral artery to the descending aorta and a stiff wire was passed through the sheath.
The Relay Plus® stent graft was selected in this case since it consists of an outer hard sheath covering a flexible sheath in which the stent graft is compressed (Fig. 5).

The Relay Plus® delivery system. The stent graft (black triangle) is compressed in the inner flexible sheath (white arrow), and also incorporated into the outer sheath (black arrow).
In conclusion, in a patient with severe aortic angulation that made it difficult to perform TEVAR, we successfully completed the operation by the addition of a stiff wire with a stiff wire.
Additionally, our technique can be applied in endovascular operations such as transcatheter aortic valve implantation.
Conflict of Interest Statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}