





Abstract
A 59-year-old man fell off a 60-cm-high step, with his ankle in a twisted position, and sustained a closed fracture of the medial malleolus, with an ipsilateral complete Achilles tendon (TA) rupture. The TA rupture was initially missed but diagnosed by ultrasound examination, 2 weeks post-operatively. The ankle fracture was diagnosed from routine radiographs. Such a combination of injuries has been reported infrequently in the literature, but significant similarities have been described in the mechanism of injury and fracture patterns. Nevertheless, three of five reported cases with combined medial malleolus fractures were initially misdiagnosed.
Ankle fractures and TA ruptures are common as isolated lesions. However, their association in the same injury is infrequent, and there are only a few case reports [1–5]. More frequently, ankle fractures have been described in association with tendon ruptures, such as the tibialis posterior [6] and the flexor hallucis longus [7]. Such lesions were shown to be secondary to entrapment of the tendon in the fracture site, and the majority were recognized only at the time of open reduction and internal fixation of the ankle fracture. A different mechanism of injury has been reported when the TA rupture is associated with an ankle fracture, and there is a high chance of misdiagnosis for such injuries [1–4]. We are reporting this combination of injuries because of its relative uncommonness in the literature and to summarize the features to be seen on initial injury radiographs to minimize misdiagnosis of these combined injuries.
Case report
A 59-year-old man came to the emergency department with a painful left ankle after twisting his foot following an unexpected fall from a 60-cm step. His forefoot landed first, followed by lateral foot adduction. On physical examination, there was significant oedema and palpable tenderness over the medial aspect of the left ankle, with reduced range of movement but with neuromuscular structures intact.
Plain radiographs of anteroposterior, mortise and lateral views revealed a fracture of the medial malleolus with no other bony injuries (Fig. 1). Surgery was performed with the patient under general anaesthetic in a supine position with an above-knee tourniquet. A medial incision was made along the medial malleolus, inline with the tibialis posterior tendon. The flexor retinaculum was incised in order to expose the tibialis posterior tendon. The periosteum of the posteromedial fragment was then elevated, and the tibialis posterior tendon was retracted with an intact tendon sheath posterolaterally. This enabled the reduction of the fracture under direct vision. Two 4.0 cannulated screws were then inserted with countersink to stabilize the fracture, and the periosteum was repaired over the top of the screw ends. The flexor retinaculum was then repaired meticulously, followed by subcutaneous and subarticular closure of the wound.
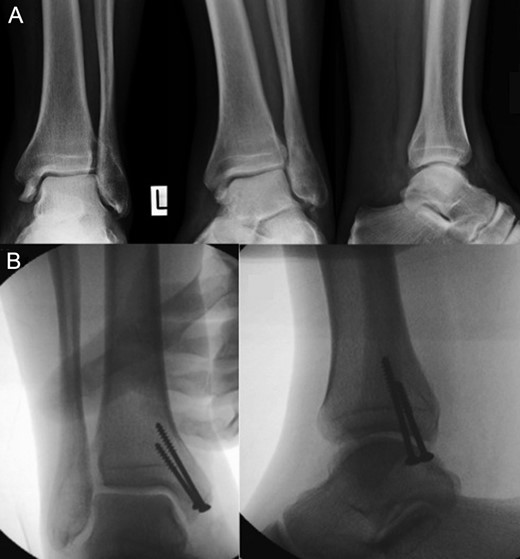
Plain radiographs of anteroposterior, mortise and lateral views revealed a fracture of the medial malleolus with no other bony injuries. A (above): before surgery, B (below): after surgery.
Two weeks post-operatively, the patient attended a follow-up clinic, complaining of pain over the TA. A ruptured TA with a minimal gap was diagnosed after ultrasound examination. The ruptured TA was managed non-surgically with a below-knee plaster for 8 weeks. At a 12-month follow-up, the patient was asymptomatic with a full range of active and passive ankle motion. Plantar flexion strength was judged equal to the opposite side on clinical examination.
Discussion
Moritz [8] commented that for TA ruptures associated with skiing injuries, a non-displaced medial malleolus fracture occurs occasionally, but no details were available in their reports. However, to support their assertion, Lugger et al. reported on a series of injured alpine skiers collected mainly in the 1960s and found a 5.3% incidence of medial malleolar fractures in those alpine skiers also treated for a TA rupture [9]. However, this injury is rare in the skiing population nowadays, due to modified skiing boots that stop ankle motion and prevent any excessive posterior TA stretching.
From a search of PubMed/Medline literature, there are five case reports describing an ankle fracture combined with a TA rupture [1–5]. In each case, the TA rupture was complete and the fracture was a closed oblique to vertical medial malleolus fracture, with extension into the tibia plafond in two cases. The lateral malleolus was intact in all reported cases. The mechanism of injury consistently implied a sudden excessive upward force applied to the forefoot followed by ankle hyperextension (in four cases), by hindfoot inversion (in three cases) or eversion (in one case).
In three cases, the TA rupture was initially missed, and in another case, the fracture of the medial malleolus was missed. Both diagnoses were initially made in two cases. The combination of a closed ankle fracture and TA rupture is rare, and only five individual cases have been reported in the literature. A review of these publications, along with our report, reveals obvious similarities in the mechanism of injury, the fracture pattern and the risk of one of the injuries being missed.
The initial mechanism of injury was the same in each case report and consisted of a sudden upward overloading force applied to the forefoot. This was assumed to be followed either by ankle hyperextension [3, 4] or hindfoot inversion [1, 2]. In our case, the patient clearly reported landing with his forefoot first, followed by lateral aspect of the foot with adduction (supination–adduction (SAD) Danis–Weber injury). Forceful loads applied to the forefoot have been experimentally and clinically reported to produce TA ruptures, and concomitant active stretching of the TA with an even lesser forefoot load causes TA rupture [10].
Our literature review revealed that when TA rupture and ankle fracture were combined, an oblique to vertical fracture of the medial malleolus was present. Such a fracture was found to result either from ankle hyperextension or hindfoot inversion. In either instance, a forceful overload of the forefoot preceded and was likely to have produced the TA rupture instead of a syndesmosis injury or high fibula fracture.
We therefore recommend that all patients with an SAD ankle injury (Danis–Weber SAD injury) have a thorough examination of the TA. Additionally, all patients presenting with TA rupture should have routine anteroposterior and lateral radiographs of the ankle to rule out an associated medial/posteromedial malleolar fracture. Any history of significant overload trauma to the forefoot should alert physicians to consider the possibility of these combined injuries. In addition, in any case of trauma, a thorough and systematic examination should be performed before a temporary splint is applied.
Conflict of Interest Statement
None declared.

{kind=link}