





Abstract
The aim of this case report was to highlight the application of magnetic resonance imaging (MRI) in elucidating serious and occult injuries in a single case of hyperflextion injury of a patient cervical spine (C-Spine). A chart and radiology review was performed to establish the sequence of care and how the results of imaging studies influenced the clinical management in this trauma case. Plain radiographs and computed tomography (CT) imaging modalities of the C-Spine revealed bilateral C4/C5 facetal subluxation with no obvious fractures; however, the MR imaging of the C-Spine revealed a non-contiguous and occult injury to C6/C7 disc with a posterior annular tear and associated disc extrusion. This altered the operative intervention that was initially planned. MR imaging proved an invaluable diagnostic addition in this particular case of cervical trauma in a rugby player following a hyperflextion injury, by revealing a serious non-contiguous and occult injury of the C-Spine.
INTRODUCTION
This case report describes an unstable ligamentous injury of the cervical spine, secondary to trauma suffered during an amateur rugby match. The proportion of these cervical spine injuries to be purely ligamentous after blunt trauma has been shown to be 0.6%, with half of this population presenting with neurological deficit [1]. Literature surrounding the incidence of cervical spine injury and associated spinal cord injury (SCI) is reported between 0.8 and 13 times per 100 000 players per year [2–4]. Rugby Union Football is a popular sport played worldwide. Injury levels amongst players remain high due to the physical demands of the sport. Fuller et al. estimated the incidence of spinal injuries to be 10.9 per 1000 player hours, in professional rugby [5]. In an Irish study reviewing 10 years of sport-related spinal injuries, rugby accounted for 16.3% of sports-related spinal injuries, with the majority of injuries occurred early in the season [6]. We present a case in which trimodal imaging of the injury proved valuable, in terms of operative planning.
CASE REPORT
A 33-year-old male was playing rugby union for his local club at the time of the injury. He was driving a Ruck when he collided with another player's chest. A ruch is defined as by the International Rugby Board (IRB) as a ‘phase of play in which one or more players from each team, who are on their feet, in physical contact, or close around the ball on the ground’ [7]. In this driving Ruck, the patient suffered a hyperflextion injury on his neck. Immediately subsequent to the injury, he experienced full body paraesthesia, noting that he had ‘pins and needles’ in his hands and feet, which resolved after 5 min. There was no loss of consciousness or head trauma. He was placed under full spinal precautions and transferred to the local Orthopaedic unit.
On arrival in the emergency department, ATLS protocol was followed. A logroll of the patient revealed cervical spine (C-Spine) tenderness without further spinal tenderness. Initial clinical examination did not elicit any neurological deficit.
The lateral C-Spine X-ray, taken as part of the trauma series, showed C4–C5 subluxation, grade 1 anterolesthesis and an acute 30° kyphotic deformity at C4/5 level through the disc (Fig. 1).

Lateral C-Spine radiograph showing bilateral C4/5 subluxation.
The patient was maintained in triple immobilization and a computed tomography (CT) scan was obtained, this revealed bilateral C4/5 facetal subluxation with no obvious fractures (Fig. 2).

Sagittal CT scan images showing a pure soft tissue bilateral C4/5 Subluxation with bilateral ‘Naked Facet’ sign.
An orthopaedic consult was sought, the working diagnosis was a high-grade cervical sprain with compromise of the posterior ligamentous complex, bilateral facet joints capsules and potentially posterior longitudinal ligament (PLL). Ultimately, to further elucidate ligamentous component of this injury and rule out disc herniation into the spinal canal, a magnetic resonance image (MRI) of the C-Spine was requested.
The MR of the C-Spine revealed C4/C5 subluxation (flexion–distraction injury) with total rupture of posterior ligamentous complex including PLL with acute traumatic disc herniation at C4/C5 level causing significant narrowing of the spinal canal at the level but no evidence of cord signal changes. Partial injury to Nuchal ligament with an acute injury to C6/C7 disc with posterior annular tear with disc extrusion, almost sequestration behind vertebral body of C7 towards left C7/T1 neural foramen, was also noted (Figs 3–5).
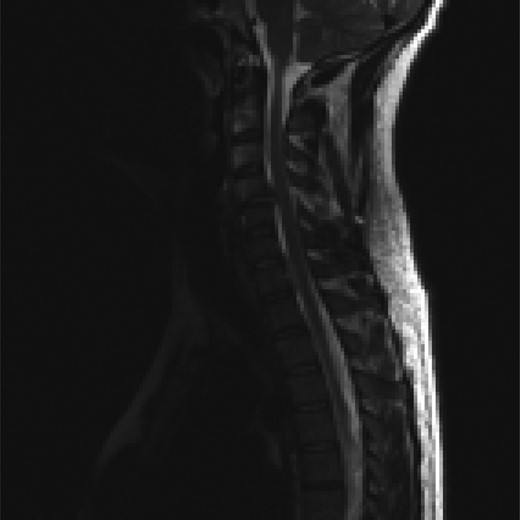
Sagittal T2-weighted MRI images showing a disc herniation at C4/5 and a non-contiguous disc extrusion at C/67 behind the vertebral body of C7.
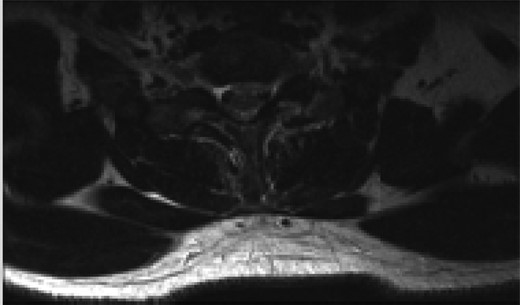
Axial T2 MRI image at C4/5 level showing central disc herniation.
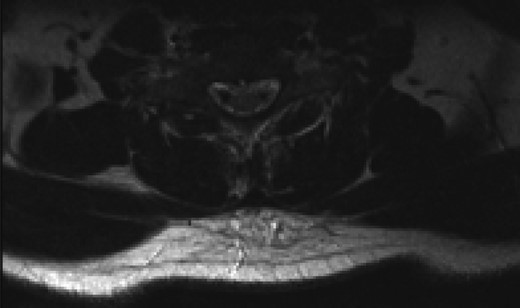
Axial T2 MRI image at C6/7 level showing central annular tear with left paracentral disc extrusion behind the C7 vertebral body.
The impression of the Spinal Service was that this was an unstable ligamentous injury of the C-Spine and would require operative intervention with an anterior cervical discectomy (ACDF) for both levels with a possible C7 corpectomy to extract the herniated C6/7 disc fragment. This was discussed with the patient and consent was given. This differed from the initial surgical plan, which was planned for a single-level surgery based on the CT findings.
The patient underwent an awake fibre-optic intubation and was placed supine on a Mayfield frame. The subluxation of the C-Spine was reduced with 10 lbs of traction. Neurology noted to be stable after reduction. General anaesthesia induced and a standard left Smyth/Robinson approach taken to anterior cervical spine with level C4–C7 exposed and confirmed on image intensifier. Surgery was performed under full spinal cord monitoring (SCM). The operative team proceeded to perform a discectomy at C4/C5, with a noted tear in the PLL. Fragments from the canal where extracted with the aid of a microscope. Then the team moved to repeat a discectomy at C6/C7, with a small midline tear in the PLL noted. A large fragment was extracted from the canal. Subsequently satisfactory decompression of the cord was achieved and stable somatosensory evoked potentials (SSEPS) and motor evoked potentials (MEPS). Standard fusion was done using a polyethyl ethylketone (PEEK) cage filled with biphasic calcium phosphate (BCP) and a single-level anterior locking plate was employed (Figs 6 and 7).

Lateral C-Spine radiograph showing realignment of C-Spine.
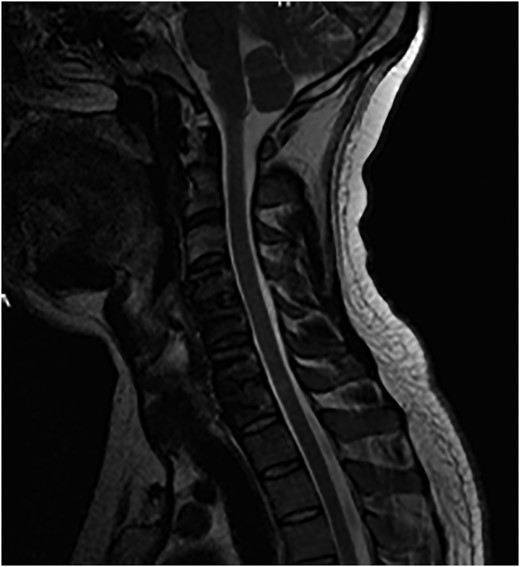
Sagittal T2-weighted MRI images showing decompression of the cord.
Patient had an uncomplicated post-operative recovery and was discharged from the hospital on day 3.
DISCUSSION
The phases of play in which the majority of cervical spine injuries occur has changed according to the literature, with more occurring in the tackle during open play since 2000 [8]. The mechanism by which cervical spine injuries occur in rugby is subject to current academic debate. Kuster et al. [8] have proposed that these injuries are due to axial compression and associated buckling of the vertebral column, drawing upon case reports and experimental cadaveric studies. Dennison et al. [9] state the hyperextension model for cervical spine injury in rugby is supported with biomechanical studies displaying that flexion moments combined with axial compression and anterior shear forces can result in facet dislocations in the lower cervical spine. Our patient has not returned to play rugby since his injury. In this case, the patient suffered a hyperflexion injury while playing amateur rugby. He suffered a C4/5 severe ligamentous injury with subluxation and a disc herniation associated with an extrusion of the disc at C6/7, which was only detected with MRI. The MRI of the C-Spine displays a pure soft tissue disc herniation at the non-contiguous level in the sub-axial cervical spine, with associated injuries giving rise to an unstable ligamentous injury of the C-Spine requiring operative intervention. In conclusion, Rugby Football Union is a common and popular sport, in which cervical spine injuries are occurring. We have described a unique cervical spine injury suffered during a rugby game and the usefulness of trimodal imaging in this case in fully characterizing the patient’s injury.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}