





Abstract
A 61-year-old woman presented to the gynecology department with complaints of atypical genital bleeding. Magnetic resonance imaging revealed a localized urethral tumor extended to vagina. Histological test of the biopsy tissue of the mass suggested the adenocarcinoma. The patient was performed the fenestration of the anterior vaginal wall 15 years ago. Under the diagnosis of urethral diverticular adenocarcinoma, we performed standard open total cystectomy with lymph node excision and ileal conduit. We could not establish a diagnosis of urethral diverticulum from the histological test; however, we clinically diagnosed as urethral diverticular adenocarcinoma. Because carcinoma arising from urethral diverticula is reported, a close long-term follow-up for the recurrence or generation of malignant tumors by genitourinary examinations or images is necessary, for the patient with urethral diverticula.
INTRODUCTION
Urethral diverticular adenocarcinoma is a rare cancer found in female patients, presenting only 5% of female urothelial cancers. We report a case of a urethral diverticular adenocarcinoma after the fenestration of the anterior vaginal wall for pelvic floor abscess.
CASE REPORT
A 61-year-old woman presented to the gynecology department with complaints of atypical genital bleeding. Vaginal examination revealed an elastic-hard mass beneath the anterior vaginal wall. Magnetic resonance imaging (MRI) revealed a localized urethral tumor extended to vagina (Fig. 1). Histological test of the biopsy tissue of the mass suggested the adenocarcinoma. Computed tomography did not reveal any evidence of metastasis. Under the diagnosis of urethral tumor, the patient was referred to our department. Because the fenestration of the anterior vaginal wall was performed under the diagnosis of the abscess in the pelvic floor for the patient ∼15 years ago and the histological test demonstrates the adenocarcinoma, we suspected a urethral diverticular adenocarcinoma.
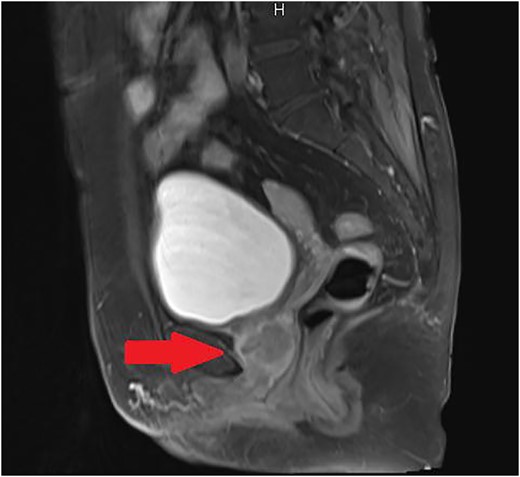
Sagittal T2-weighted MRI of the pelvis revealed a localized urethral tumor extended to vagina.
On admission, we performed standard open total cystectomy with lymph node excision and ileal conduit. The resected specimen showed the mass on the anterior vaginal wall (Fig. 2). Histopathological examination of the specimen showed adenocarcinoma tumor that continues to anterior vaginal wall, but urethral diverticular wall could not be identified (Fig. 3). We could not establish a diagnosis of urethral diverticulum; however, we clinically diagnosed as urethral diverticular adenocarcinoma. The proximal margin was negative, and all lymph nodes were negative. Because the post-surgical course was uneventful, the patient was discharged from our hospital on Day 27 post-surgery. The patient is doing well without recurrence or metastasis for 12 months.
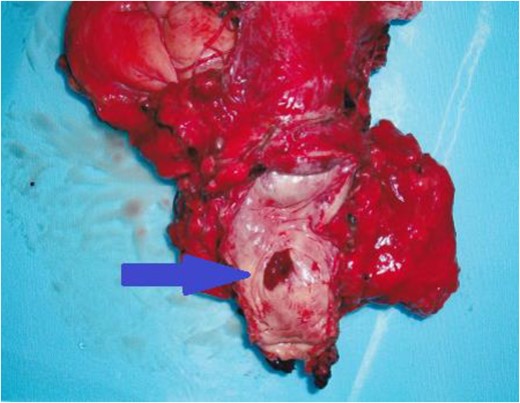
The resected specimen showed the mass on the anterior vaginal wall.
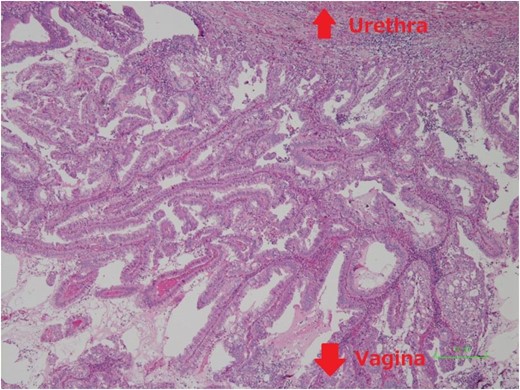
Histopathological examination of the specimen showed adenocarcinoma tumor which continues to anterior vaginal wall, but urethral diverticular wall could not be identified.
DISCUSSION
Urethral diverticular carcinoma was first reported in 1951 [1]. It is a rare cancer found in female patients. To date, there are less than 60 reported cases of urethral diverticula carcinoma, including adenocarcinoma and squamous cell carcinoma [2]. Anil et al. insisted that identified invasive carcinoma arising from urethral diverticula is ∼6% [3]. Because there are few case reports, this disease entity is poorly understood. Urethral bleeding is the most common presenting symptom, occurring in 51% patients. A painless growth, found initially as either an anterior vaginal mass or a urothelial obstruction, was present in 24% patients. Localized irritation, pain and an ulcer also are presenting symptoms [2]. Therapy for urethral diverticular carcinoma consists of local excision such as diverticulectomy or more aggressive therapy such as definitive radiation therapy or radical cystourectomy with pelvic lymph node dissection.
In our case, it is possible that drainage treatment was performed for urothelial diverticulum ∼15 years ago. Patients with urethral diverticula often present with a variety of nonspecific lower urinary symptoms such as frequency, urgency, localized pain or dysuria. Approximately 4% cases of female urethral diverticulum cause urinary retention [4]. An asymptomatic patient with urethral diverticulum can be managed by observation. On the other hand, the first and most common choice of treatment for symptomatic urethral diverticulum is complete vaginal excision. However, because of several risks and the high recurrence rate of complete vaginal excision, we have advocated that the management by transvaginal drainage could be the appropriate treatment for urethral diverticulum on the past published case report [5]. This procedure is effective and conservative with few complications, but we should not forget very rare cases of carcinoma arising in urethral diverticula have been reported. In this case, if the urethral diverticulum had removed completely 15 years ago, the generation of malignant tumors might have been avoidable. Anyway, for the patient with urethral diverticula, close long-term follow-up for the recurrence or generation of malignant tumors by genitourinary examinations or images is necessary.
CONFLICT OF INTEREST STATEMENT
None declared.
ACKNOWLEDGEMENTS
I am very glad to the Ehime Urological Association for making my case report passible by the financial support.

{kind=link}
{kind=link}
{kind=link}