





Abstract
Coronary artery aneurysm is a rare clinical entity encountered incidentally 0.3–5% among patients who undergo coronary angiography. Even giant coronary artery aneurysm is much rarer with an incidence of 0.02% among all atherosclerotic cases. Due to rare occurrence and lack of controlled trials, clinical presentation, prognosis and management of giant coronary artery aneurysm are under controversies in the literature. We report a 43-year-old male patient admitted to our hospital with a typical chest pain associated with ST elevation changes in anterior chest leads and elevated cardiac enzymes. Coronary angiography of the patient revealed a large (1.5 cm × 3 cm) aneurysm of proximal left anterior descending coronary artery. We performed a successful surgical excision and coronary bypass surgery. The patient had an uncomplicated course.
INTRODUCTION
Coronary artery aneurysm is a rare clinical entity with an estimate incidence of 0.3–5% among patients who undergo coronary angiography [1]. It is usually presented with myocardial ischemia due to rupture or distal embolization [2]. Giant coronary artery aneurysm is defined as a coronary dilatation that exceeds by four times or has a diameter exceeding 8 mm, and is under controversies in the literature [3]. Giant coronary aneurysm is even less common in only 0.02% of all atherosclerotic patients [3]. Due to lack of clinical trials and its rarity, clinical presentations and the best strategic management of it are under controversies in the literature.
CASE REPORT
A 43-year-old male patient was admitted to our hospital for a new sensation of tightness in his chest. He also complained of chest pain in retrosternal region radiating to his left arm and aggravated with walking, lasting ∼30 min. He did not have any medical history of hypertension or diabetes in his last check-up visit, but he was smoker. He had family history of coronary artery diseases in his father who died in the age of 62 years. On clinical examination, he was hemodynamically stable without any pathological findings. His height was 173 cm, and his weight was 75 kg. The electrocardiogram initially showed an ST elevation of >0.2 mV in anterior chest leads from isoelectric baseline. Reciprocal changes were seen in inferior limb leads, consistent with ST elevation myocardial infarction (Fig. 1). During monitoring in the next 10 min of arrival, ST elevation in anterior chest leads subsided, and the patient was treated as an ordinally unstable angina. Routine lab tests showed positive troponin, and echocardiography showed an ejection fraction of 55% without any valvular abnormalities.

Electrocardiogram of the patient during the early time of admission showed ST elevation myocardial ischemia.
Coronary angiography was performed next day. It revealed a large (1.5 cm × 3 cm) aneurysm in the proximal part of left anterior descending coronary artery (LAD) with significant stenosis at its mid part (Fig. 2). The patient underwent successful resection of the giant aneurysm by coronary artery bypass surgery, using left internal mammary artery to bypass LAD. The patient had a usual course of hospitalization and discharged without any complications. At 6 months of follow-up, he has been asymptomatic.
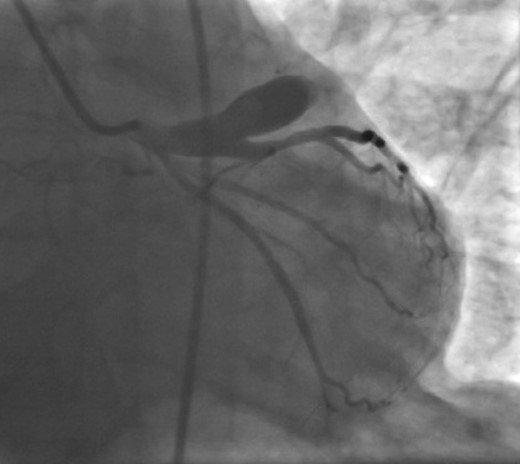
Coronary angiography showing giant coronary aneurysm originating from the proximal part of left anterior descending coronary artery.
DISCUSSION
Giant coronary artery aneurysm is defined as a coronary dilatation that exceeds at least four times of the reference diameter or has a diameter exceeding 8 mm [3]. It is a rare coronary pathology, most commonly due to atherosclerotic origin. Also, other causes include the Kawasaki disease, autoimmune disorders and angioplasty complications [4]. Only a few cases have been reported, and due to its rarity, clinical manifestations and the best strategic management are under discussion in the literature.
Up to one-third of the patients with coronary artery aneurysms may present with angina pectoris or myocardial infarction or sudden cardiac death and congestive heart failure [3]. In our case, we found ST elevation changes in the electrocardiogram during the early time of the admission, consistent with ST elevation myocardial infarction. Emergent thrombolysis in this case could be detrimental as ruptures of coronary artery aneurysms also have been described. Subsequent tamponade and/or sudden death may occur [5]. Although such cases have not been assumed, it could bring challenges in recent guidelines for treatment of such patients.
Surgery is the best preferred management for giant coronary artery aneurysms, which requires median sternotomy and coronary revascularization [3, 4]. Due to lack of controlled trials, prognosis of giant coronary artery aneurysm is under controversies. During 6 months of follow-up, our patient remained asymptomatic without any limitation in his quality of life. The overall 5-year survival is reported to be 71% [3, 5]. Giant coronary artery aneurysm is a rare pathology of coronary vessels due to atherosclerosis or other causes. It may manifest with angina pectoris. It should be considered in the differential diagnosis of ischemic heart disease. For the exact diagnosis, coronary angiography should be required, and emergent surgical management should be planned for the best outcomes. Written informed consent was obtained from the patient for publication of this case report including the pictures.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}