





Abstract
Metal-on-metal (MoM) bearing in total hip replacement (THR) has a high failure rate due to adverse reaction to metal debris (ARMD). There is a spectrum of soft tissue and bony changes in ARMD including muscle necrosis and osteolysis. In our institution, more than 1500 MoM THRs were implanted since 2003. Recently, we have revised significant numbers of these. We report our experience and management of a mode of failure of MoM THR that has been infrequently reported—the distal femoral stem fracture. We report on two patients who presented with worsening pain attributable to fracture of the femoral stem. Severe femoral osteolysis led to loss of proximal stem support and eventual fatigue fracture of the component. Both patients were revised employing a posterior approach. Bone trephine was used to extract a well-fixed distal stem fragment without any windows. Both patients had successful outcome after revision with excellent pain relief and no complications.
INTRODUCTION
Metal-on-metal (MoM) bearings in total hip replacements (THRs) had been used widely due to their perceived advantage of low wear and large stable bearing. It has become apparent that the failure rate with large metal bearings is associated with a high rate of serious complications including osteolysis, tissue necrosis and formation of pseudo tumours [1–3]. Many health regulatory authorities issued health warnings, recalled those implants and recommended close surveillance of patients with these implants [4]. In our institution, more than 1500 MoM THRs were implanted. Dedicated MoM follow-up clinics were set up to monitor those affected in accordance with the UK Medicine and Healthcare products Regulatory Agency (MHRA) guidelines. Femoral stem fracture is rare in primary implants. Here, we report two cases of distal stem fracture in primary MoM THR and the operative technique used to retrieve well-fixed distal component.
CASE REPORT
Case 1
A 74-year-old man presented to our MoM surveillance clinic with sudden onset of severe left hip pain. Five years prior to presentation, he had undergone a left MoM THR with a Profemur stem and Procotyl cup (Wright Medical Ltd, UK). The patient also had undergone a right THR with a similar prosthesis 6 years prior to this presentation. One year prior to presentation, he was noticed to have raised metal ions (cobalt and chromium) and X-ray of his left hip showed radiolucent lines in Zones 1 and 7. While awaiting an MRI scan, he contacted our clinic complaining of sudden severe left hip pain without history of trauma. X-ray of his left hip showed a distal stem fracture (Fig. 1a). He was admitted from the clinic and his left hip was revised with ceramic on polyethylene bearing using Exeter stem and Trident cup (Stryker UK Limited; Fig. 1b).
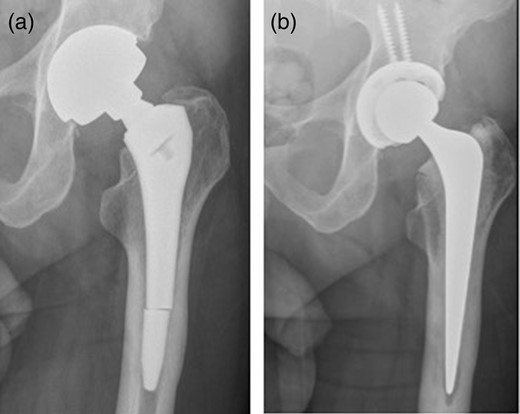
(a) Distal stem fracture of left hip prosthesis. (b) Post-revision X-ray.
Case 2
An 83-year-old female presented to our MoM for a routine review. Fourteen years previously, she had undergone a bipolar hemi-arthroplasties with a Furlong hip system (JRI limited UK). The bipolar hemi-arthroplasties was revised 6 years previously due to increasing hip pain and protrusion. At revision to THR, an R3 acetabular cup with a metal liner (Smith & Nephew, UK) was used retaining the primary stem. She described a 2-month history of a significant increase in pain over her right hip. There was no history of trauma or fall. X-rays showed a fracture through the stem of her right femoral component with radiolucent line in Zones 1, 2, 6 and 7 (Fig. 2a). She was admitted from the clinic and right hip was revised with ceramic on polyethylene bearing using Exeter stem and Trident cup (Stryker UK Limited; Fig. 2b).
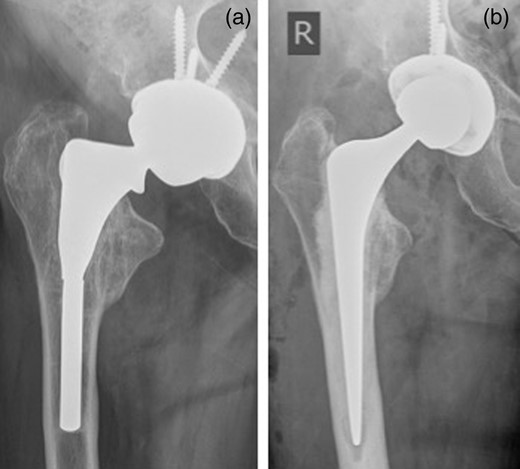
(a) Fracture through the stem of right femoral component. (b) Post-revision X-ray.
In both cases, there was evidence of significant osteolysis in the proximal femur (Fig. 3); microbiological testing of intraoperative specimens was sterile. The proximal part of each stem was loose and easily removed (Fig. 4). The distal stems were well fixed and were extracted antegrade using trephine (DePuy Moreland Cementless Extraction System, Leeds, UK) without osteotomy. In this technique, the trephine is used to ream the cement mantle around the distal portion of the stem till either the stem is trapped within the trephine, and can then be removed with it, or an appropriate space is made for a grasper to be introduced to remove the stem. The outcome was excellent for both cases with immediate pain relieve and no early complications. The oxford hip scores were 43/48 for Case 1 at 5 months and 36/48 for Case 2 at 4 months.
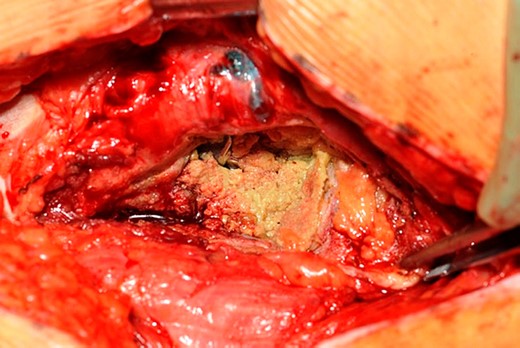
Metalosis in Case 1.

Broken stem in Case 1.
DISCUSSION
Fracture of the femoral stem was a common complication of hip prosthesis during the 1970s and early 1980s. Due to better implant design and stronger metal alloys, the incidence has significantly decreased [5] to an estimated rate of 0.27–2.3% for both cemented and cementless prosthesis [6, 7]. Multiple factors have been reported to correlate with increased incidence of femoral stem fractures including increased patient weight, high levels of activity, undersizing of stem, stems with decreased cross-sectional area and long necks, various positioning of the stem and, most importantly, inadequate proximal support for the implant in the proximal femur due to either cement debonding proximally in cemented stems or osteolysis [8, 9]. In MoM arthroplasty, osteolysis is thought to be the end result of chronic release of wear nanoparticles and high levels of metal ions, particularly cobalt, causing cell death, local soft tissue destruction and osteoblastic activity impairment [4]. In our institution, over the last few years, we have revised significant numbers of these patients with adverse reactions to their metal bearing hips. We report two cases of distal stem fracture in two patients with primary stems and MoM bearings. Both patients had radiological and intraoperative evidence of osteolysis secondary to adverse reaction to metal debris. Stem failure can be explained by the ‘bending cantilever’ phenomena where proximally there is loss of stem support while distal portion of the stem remains securely fixed subjecting the stem to cantilever forces resulting in metal fatigue and subsequent fracture. Extraction of well-fixed distal femoral broken fragment has been achieved traditionally via cortical window or femoral osteotomy to allow access to femoral canal and removal of intact component. In our cases, well-fixed distal components were removed using a trephine (DePuy Moreland Cementless Extraction System) without need for any femoral windows as described by Vasireddy et al. [10]. In conclusion, a sudden increase in symptoms in the presence of proximal femoral osteolysis should lead to consideration of implant fracture. The extraction of well-fixed distal portion could be achieved using trephine without the need for femoral windows.
FUNDING
No funding or financial support was obtained for this study.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}