





Abstract
We report a recurrent Piriformisc muscle syndrome after surgical release. After the primary neurolysis, a second operation was performed to release adhesions. This case shows a different type of sciatic nerve entrapment by an abnormal thin muscle slip. Results of the revision surgery guide us to the point that revision surgery for Piriformis muscle syndrome should be meticulously selected, and after considering medical and interventional therapies.
INTRODUCTION
Piriformis muscle syndrome was first described by Yeoman (1928) [1]. This syndrome is sometimes overlooked as a cause of radiating lower extremity pain. First-line treatment is non-operative strategies. Surgical release is considered for individuals who do not respond to conservative methods. Recurrence after surgery for Piriformis muscle syndrome has been reported by Kobbe et al. [2], and to the best of our knowledge, this is the second study addressing this subject.
CASE REPORT
A 28-year-old house wife presented with a 2-year history of left lower extremity radicular pain. She did not experience low back pain or dyspareunia at any point. The associated complaints were tingling and numbness of left foot. Her symptoms aggravated with standing, sitting and lying on her left side. She received a full course of conservative treatment, which did not bring about relief of pain.
On physical examination, she had positive Freiberg's and Pace's signs tests. Left-sided gluteal atrophy was noticed. A localized tenderness over the left gluteal area was present. Patellar and Achilles tendon reflexes and lumbar range of motion were normal. No tenderness over vertebras was detected. She had negative straight leg raising and Patrick's test. A left-sided S1 distribution paresthesia was detected. The lower extremity muscle power was intact.
She underwent extensive imaging studies including left thigh, pelvis and lumbosacral magnetic resonance imaging (MRI) and X-rays that revealed no specific finding. Electromyography-nerve conduction velocity tests showed delayed H reflex and left tibial mononeuropathy (partial nerve conduction blocks features). Additionally, polyphasic motor units were reported for lower limb muscles. Taking into account the clinical picture, imaging studies and electrodiagnostic studies, Piriformis muscle syndrome was considered as a possible diagnosis.
In right down decubitus position, a left curvilinear incision was made over gluteal area. A 3- to 4- mm width muscle bundle pierced sciatic nerve transversely; 4 cm after the nerve exited sciatic notch (Figs 1 and 2). The muscle bundle was cut and nerve released. After complete hemostasis and irrigation, wound was closed in layers.
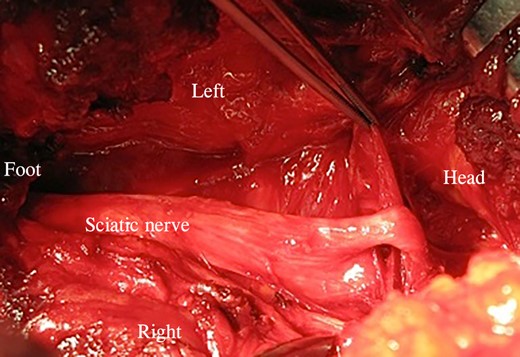
The forceps shows the muscle slip.
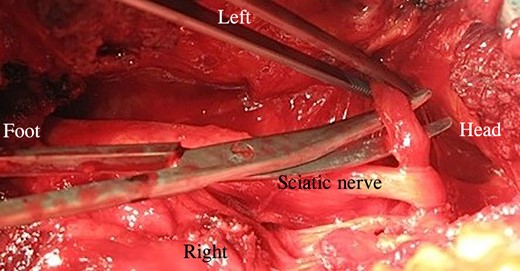
Surgical scissor shows how stretching the muscle bundle affected sciatic nerve.
The patient recalled no pain or sensory complaints during the immediate postoperative period. Eight months after the operation, she started experiencing the recurrence of her primary symptoms but with less intensity (VAS 3/10). The pain and sensory problems intensified over months, which did not respond to conservative measures. MRI was done, which did not reveal any specific finding.
Second operation was performed that included reopening of the previous incision and sciatic nerve exploration. A severe adhesion around sciatic nerve was observed. Neurolysis was performed, and the nerve was released along its path. To prevent further scar formation, a fat sleeve was placed around the area where sciatic nerve had adhesions.
The patient recalled an immediate postoperative pain that was as severe as before the operation period. We started medical therapy with Lyrica and Gabapentin, Cymbalta, Perphenazine and aquatherapy. During our last interview with her, she complained of the pain (VAS 5/10) and sensory problems.
DISCUSSION
Piriformis muscle has been reported in 22% of population [3] and accounts for 5–6% of cases who are referred for back and leg pain [4]. The causes attributed to this syndrome have been classified as buttock trauma, compression and overuse [5] that may lead to muscle hyperthrophy, inflammation and irritation. Congenital abnormalities between Piriformis muscle and sciatic nerve could also be a cause for this syndrome [6]. Treatment of Piriformis syndrome starts with conservative measures. Cases who do not demonstrate improvement with conservative methods or interventional treatments could be candidates for surgery [7].
To the best of our knowledge, recurrent piriformis syndrome has been documented by Kobbe et al. [2]. Our patient similar to the cases reported by Kobbe et al. [2] had an anatomical variation of piriformis muscle and sciatic nerve. During revision surgeries performed by Kobbe et al., scar tissues around sciatic nerve were encountered and released, the same finding that was observed during our revision surgery. Kobbe et al.'s cases had complete post-revision surgery symptom relief, a result that we failed to achieve. At their 3-year follow-up, one of their patients was completely pain-free and another complained of residual left gluteal and left lower extremity pain. Our patient had some residual left gluteal and left lower extremity pain and sensory complaints at 2-year follow-up from her revision surgery.
In conclusion, we recommend an intensive course of conservative treatment with special focus on physiotherapy before proceeding with revision surgery. Additionally, interventional methods should be considered in cases that show insufficient response to the primary conservative methods. Choice of barriers for scar prevention is another issue that must be carefully selected during revision surgeries.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}