





Abstract
Chilaiditi's sign and syndrome seem similar but are actually different entities, difficult to distinguish from each other. A 60-year-old female presented with a clinical scenario of intestinal obstruction, which was thought to be Chilaiditi's syndrome because of the unusual impression of gas under the diaphragm, but was confirmed as Chilaiditi's sign after laparotomy. The interposition of dilated small bowel loops below the diaphragm due to distal obstruction somewhere else can also produce a Chilaiditi's sign.
INTRODUCTION
Chilaiditi's sign is an incidental radiographic finding of subdiaphragmatic radiolucency due to the interposition of a bowel segment between the liver and the diaphragm [1]. However, Chilaiditi's syndrome refers to a clinically symptomatic patient along with the presence of the radiographic findings: the symptoms resulting from the interposition itself, which can range from intermittent, mild abdominal pain to acute intestinal obstruction, constipation, chest pain and breathlessness [2–4]. The syndrome was first described in 1910 by Demetrius Chilaiditi [5]. Here, we report a case in which we thought of Chilaiditi's syndrome because of the impression of gas under the diaphragm associated with features of intestinal obstruction, which eventually turned out to be Chilaiditi's sign due to Richter's hernia at the femoral canal.
CASE REPORT
A 60-year-old female of Aryan ethnicity presented to our emergency department with history of not passing stool and flatus for 3 days, bilious vomiting and abdominal distension. She was obese, her vitals were relatively stable and her abdomen was distended and tense. Her liver dullness was obliterated, and she had a tympanitic note on percussion and mild tenderness all over the abdomen. Rectal examination showed an empty rectum.
Plain supine abdominal radiograph showed features of small bowel obstruction. However, a plain chest radiograph taken in erect position showed radiolucent shadow under the right dome of the diaphragm, first simulating pneumoperitoneum (Fig. 1). The impression of free gas under the diaphragm was very much supported by the clinical finding of obliterated liver dullness. However, on careful examination of the radiograph, few semilunar radio-opaque linings could be seen, which could be walls of bowel loops (Fig. 2). She was diagnosed as acute intestinal obstruction, probably Chilaiditi's syndrome: we thought of obstruction due to herniation into the hepatodiaphragmatic space.
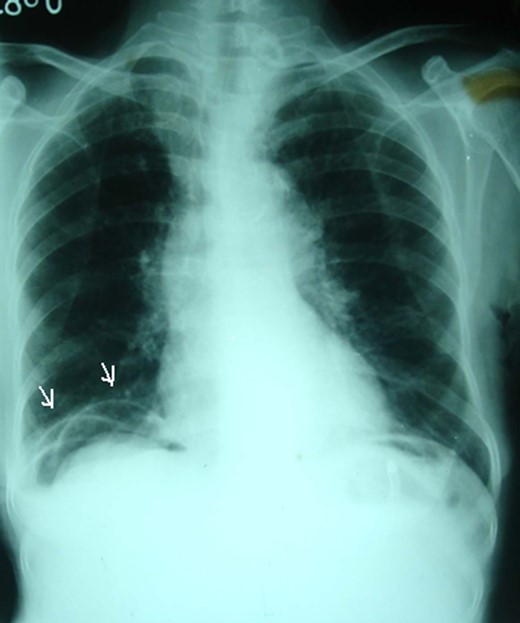
A plain erect chest radiograph showing appearance of radiolucency under the right hemidiaphragm (arrows).

Careful examination showing semilunar opaque lines which were walls of small bowel loops (arrows).
She underwent an exploratory laparotomy, in which we found distal ileal obstruction due to Richter's type strangulated right-sided femoral hernia, along with proximal multiple distended bowel loops and distal collapsed ileal loops. Few distended small bowel (ileal) loops had slided between the liver and the anterior parietal wall to reach below the right dome of the diaphragm (hepatodiaphragmatic space). They were retrieved down, and there were no any adhesions; the liver was of normal size and anatomy. The strangulated segment was released from the hernia with resection of the gangrenous segment of the ileum; decompression of the rest of the small bowel was done followed by end-to-end anastomosis and repair of the femoral hernia. She recovered well after the operation without any complications and is well till 1 year of follow-up. The radiographic findings were concluded to be Chilaiditi's sign due to Richter's type femoral hernia and not Chilaiditi's syndrome, because bowel obstruction was not due to the infradiaphragmatic pathology, and it remained an incidental finding.
DISCUSSION
Chilaiditi's sign is defined as the interposition of bowel loop (usually colon, sometimes small bowel) and the liver below the right hemidiaphragm. It is mostly an incidental finding with a rare reported incidence of 0.025–0.28% in abdominal or chest radiographs [1]. On the other hand, Chilaiditi's syndrome may involve symptoms such as abdominal pain, chest pain, breathlessness and constipation; even acute intestinal volvulus due to such pathology has also been reported [4]. The clinical features are implicated due to the interposition itself. The present case features a lady who had presented with obstruction, and based on radiographs was suspected to be due to Chilaiditi's syndrome. However, on laparotomy, the cause was a Richter's type femoral hernia that gave rise to Chilaiditi's sign due to sliding of the small bowel into the hepatodiaphragmatic space. Our literature search has revealed only six reports of Chilaiditi's sign involving the small bowel till date [3, 6–10]. An association of Chilaiditi's sign with either Richter's or femoral hernia has never been reported in the literature till date; and this report is the first of its kind.
Various predisposing factors for Chilaiditi's sign have been listed, like cirrhosis, chronic obstructive pulmonary disease, pregnancy, mental disorders, obesity, primary lung cancer, diaphragmatic paralysis, postoperative adhesions, right lobe agenesis and significant weight loss [8–10]. The postulated factors are thought to be (i) a redundant bowel with long mesentery and increased mobility; (ii) an increase in the space between the liver and the diaphragm secondary to long hepatic suspensory ligaments, ascites and pregnancy; and shrinkage of the liver like in cirrhosis, which leaves adequate space for intrusion of adjacent bowel segments [2]. The present case is unique in that femoral hernia led to obstruction of the small bowel; probably the distension of the small bowel loops exerted so much pressure that they could not be accommodated in the peritoneal cavity, so they slided between the anterior parietal wall and the liver to lie in the hepatodiaphragmatic space to produce such a radiological picture of Chilaiditi's sign. A femoral hernia as the cause of intestinal obstruction was never thought of preoperatively, probably because she never gave history of any swelling at the femoral region, she was obese, and hence was missed on initial clinical examination. Management regarding classical cases of Chilaiditi's syndrome is clear: conservative for all uncomplicated cases, and surgery being indicated in cases associated with colonic volvulus, bowel ischemia, bowel obstruction and persistent pain [4, 8, 9]. During surgery, various treatment options have been described, including hepatic extraperitonealization (hepatopexy), transverse colectomy, right hemicolectomy, and colopexy [10]. In our case, retrieval of the bowel and its decompression sufficed.
Chilaiditi's syndrome and sign are related entities within a spectrum, and to distinguish them can sometimes be very difficult. Though the syndrome suggests the pathology in the subdiaphragmatic region, Chilaiditi's sign may point out to a cause that is distant from the obviously evident site, such as a femoral hernia, as in the present case.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}