





Abstract
If single adrenal metastasis surgery is well admitted, no recommendation exists about the management of a renal vein tumor thrombus, even though the actual consensual attitude consists in a nephrectomy associated to an adrenalectomy. We report, here, the case of a 74-year-old man with a suspected adrenal metastasis of a lung carcinoma associated with a left adrenal and renal vein tumor thrombus treated by adrenalectomy and renal vein thrombectomy and ipsilateral kidney sparing. The postoperative computed tomography scan showed no thrombus in the left renal vein. Doppler ultrasound performed 1 month after adrenalectomy proved a good left renal vein flux. At 36 months of follow-up, the patient is alive without signs of recurrence.
INTRODUCTION
Since the early 1980s, adrenalectomy has been shown to be a good treatment for single adrenal metastasis [1]. Indeed, adrenal metastasis surgery is proven to be a good therapy among patients in whom the previous disease, with an isolated adrenal metastasis, is controllable [2]. Studies showed good results in this surgery with increased long-term survival rates. Thus, Vivian et al. report a 30% increase in survival rates among patients who underwent surgery of a single adrenal metastasis in lung cancer [3]. Despite a lack of guidelines, surgery for isolated adrenal metastasis trends to become a reference [4] and consists in a total resection of the adrenal gland with disease-free margins.
In rare instance of adrenal tumors, a tumor thrombus can be found in the renal vein or even in the vena cava. In such a case, no recommendations are available on how to perform the adrenalectomy. The consensual therapeutic attitude consists in a one-time surgery with ‘en bloc’ resection of the tumoral vein thrombus, the adrenal and the ipsilateral kidney.
Herein, we report the case of a 74-year-old man with a single adrenal mass associated to a renal vein tumor thrombus treated by adrenalectomy, renal vein thrombectomy without ipsilateral nephrectomy.
CASE REPORT
A 74-year-old man was referred in December 2011 to our hospital for an adrenal mass, discovered during the follow-up of a pT3-N1 M0 large cells neuroendocrine lung carcinoma, treated in June 2011 by surgery. The lobectomy had been followed by four adjuvant cures of carboplatin GP 16. His main past medical history was hypertensive cardiopathy and non-insulin-dependent diabetes mellitus. On a clinical point of view, he had no symptoms and in particular no general physical deterioration. The computed tomography (CT) scan showed a left adrenal mass (7 × 10 cm enhanced with contrast) associated with a renal vein tumor thrombus (Fig. 1). A positron emission tomography scanner showed adrenal mass and renal vein tumor thrombus hypermetabolism proving their tumoral hallmarks. Surgical treatment was decided after anticoagulation treatment initiated (continuous intravenous administration of sodic heparin at the dose of 500 international unit/kg/day); after a left subcostal incision, the left colon was mobilized and the retroperitoneal space approached. Once the adrenal gland was visualized, its main vein was isolated and followed until the renal vein to localize the tumor thrombus. Using kidney cancer surgical technique for vena cava thrombectomy, we isolated all the confluents to the renal vein. After quadruple clamping (renal vein X2, spermatic vein and lumbar vein), the left renal vein was laterally opened in order to perform the thrombectomy, and the main adrenal vein was cut. Total clamping time was 12 min with no arterial clamping and no renal cooling required. The renal vein was washed with a heparinized saline solution and closed with a polypropylene 6/0 running suture. Then, the veins were unclamped, and finally the adrenal gland was removed with macroscopically disease-free margins taking away the adrenal fat along the upper renal pole capsule.
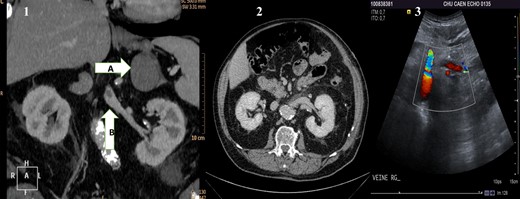
(1) Preoperative CT scan showing the adrenal mass (A) and in the renal vein a hypodense mass (B) corresponding to the renal vein tumor thrombus. (2) Postoperative CT scan showing the left kidney and its permeable vein. (3) Flow in the left renal vein on postoperative Doppler ultrasound.
The postoperative management was simple except for an Aeromonas hydrophila pulmonary infection, which was successfully treated by a 15-day cure of antibiotics. The patient was discharged on Day 15. Histopathological studies revealed a 7-cm ‘round’ cells undifferentiated tumor with a vein tumor thrombus. No adjuvant treatment was proposed because there was no relation with the lung carcinoma, and tumor's resection margins were negative. The postoperative CT scan showed no thrombus in the left renal vein (Fig. 1). Doppler ultrasound performed 1 month after adrenalectomy proved a good left renal vein flux (Fig. 1). At 36 months of follow-up, the patient is alive without signs of recurrence.
DISCUSSION
If adrenalectomy is a well-admitted treatment of single adrenal metastasis, no recommendation exists concerning adrenal masses with renal vein or vena cava tumor thrombus. Perez Utrilla et al. [5] have presented a case of an adrenal carcinoma with renal vein tumor thrombus treated by adrenalectomy, thrombectomy without ipsilateral nephrectomy. Adrenal cancer with renal vein thrombus remains an occasional pathology: Figueroa et al. described a series of 206 patients with adrenalectomy for cancer among which 6 had an adrenal vein tumor thrombus and 3, only, associated with a renal vein thrombus. In these three cases, the ipsilateral kidney was removed in the same procedure [6]. To our knowledge, our case is the first description of such a procedure with ipsilateral kidney preservation for supposed lung adrenal metastasis with renal vein tumor thrombus. Nephron sparing makes sense in the case of metastasis because good renal function permits optimal adjuvant chemotherapy and thus better survival. Indeed, Sun Youn et al. [7] reviewed 8223 cancer patients with a measurement of the serum creatinine at least once during treatment. They demonstrated that chronic kidney disease is associated with an increased risk of cancer-specific mortality. The hazard ratio was between 1.12 and 1.75 according to the level of chronic renal disease. This is not a surprising result; in 2004, Shlipak et al. [8] showed that patients with chronic kidney disease were frailer (tool to define individuals who lack functional reserve and are at risk for functional decline) than the standard population. Even though more studies are necessary, this surgery seems to be a good treatment for adrenal gland tumors with a tumoral vein thrombus.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}