





Abstract
Endometriosis is a painful disorder characterized by endometrial tissue outside the uterine cavity. It usually affects the pelvis, but in rare cases it might extend to other parts of the body. The report is based on a case of a 39-year-old woman, who presented symptoms of acute appendicitis and diagnosis confirmed with ultrasonography and a computed tomography scan procedures. Laparoscopic appendicectomy was performed. After entering the abdominal cavity, hemoperitoneum was discovered with no associated pelvic or abdominal lesions. Biopsy confirmed acute appendicitis with endometrial glands and stroma infiltrating its muscular tissue. Patient recovered without complications and was discharged 48 h after surgery. The appendix is rarely affected by endometrial infiltration. The literature describes an incidence of 0.8%, just a few cases have been associated with acute appendicitis; however, none of them are described to present hemoperitoneum, being our patient the first one reported with such complication.
INTRODUCTION
Endometriosis is the presence of endometrial glands and stroma outside the uterine cavity, affecting 5–15% of women in reproductive age [1]. It usually compromises pelvic organs, but in some occasions it has been described in some other parts of the body; except the spleen. From these extrapelvic cases, the bowel is affected in 3–37%, while the appendix only in 0.8% [2, 3].
Even though the endometriosis tends to present chronic pelvic pain, the appendicular form is most of the time asymptomatic [4]. The gold standard for its diagnosis is laparoscopy, which allows the direct visualization and removal of the lesions for histological confirmation.
This report comprises the case of a patient with appendicular endometriosis who presented acute appendicitis symptoms successfully treated with surgery and the unusual intraoperative finding of hemoperitoneum. The histopathological results confirmed the focus of endometriosis in the appendix.
CASE REPORT
A 39-year-old woman, without significant medical history, was admitted to the emergency room at the Vic University Hospital complaining of epigastric pain radiated to the right iliac fossa side and vomits starting 24 h before consultation. The patient referred to be menstruating at the time. On physical examination, she had a normal vital signs lecture and rebound tenderness at her lower right abdominal quadrant, especially in Mc Burney's point, and a positive Rovsing and Blumberg signs. Blood tests revealed anemia and a C-reactive protein level of 102 with a normal white blood cell count. Abdominal ultrasound described a small amount of free fluid on the right iliac fossa side, with slightly increased echogenicity of mesenteric fat at the same level, with no direct visualization of the appendix, and then a computed tomography scan was performed, which reported inflammatory changes on the right iliac fossa with thickened walls of small bowel, suggesting the diagnosis of appendicitis, although it could not be clearly identified.
Laparoscopic appendicectomy was performed in which the following was found: moderate hemoperitoneum (Fig. 1), edematous terminal ileum and a flemonous appendix. The macroscopic analysis of the biopsy showed an appendix of 2.8 cm of length and 0.4 cm of diameter. Microscopically, the sample presented acute and chronic serosal inflammation and endometrial glands in the apex compatible with endometrial stroma (Fig. 2).
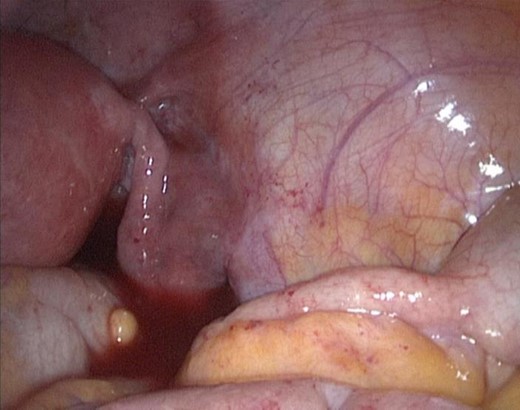
Intraoperative finding of hemoperitoneum as complication of appendicular endometriosis.
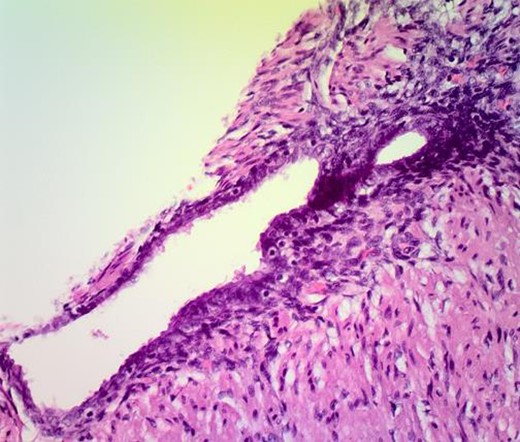
Histopathological examination of the appendix showing endometrial gland and stroma in its muscular tissue.
The patient recovered successfully from surgery and was discharged 48 h later. Six months after the surgery, she refers no abdominal pain or other symptoms.
DISCUSSION
Several conditions have been reported as possible predisposing factors for endometriosis such as race, age, body mass, alcohol and tobacco. Although currently the etiology has not been established, three theories have been proposed to explain the origin of this pathology. The first one proposes implantation with retrograde menstruation from the uterus to the abdominal cavity through the fallopian tubes. The second one, called the metaplasia theory, suggests that remaining epithelial coelomic cells, present on the peritoneal surface of the ovaries; originally dormant, activate in response to the cyclic hormonal stimulation, just like the endometrial cells normally do. The third theory, called systemic metastasis, explains that fragments of endometrial tissue embolize distant sites through blood and lymphatic circulation [5].
For this case, the authors consider as possible sources for appendicular endometriosis either retrograde menstruation, which would explain hemoperitoneum, or direct extension of possible endometriosis from the right ovary; however, appendicular lesions have been also described without any ovarian disease associated [6], as in this patient, to whom laparoscopy did not reveal other intra-abdominal or adnexal endometrial implants.
Appendicular endometriosis may be asymptomatic, being accidentally found during other pelvic pathologies surgical treatments [7], and is less frequently accompanied by nonspecific symptoms unrelated to menstrual cycle. Nonetheless, that was not the case of this patient to whom menstruation coexisted with exacerbation of the disease, as in the case reported by Uwaezuoke whose patient was in the second day of her menstrual cycle by the time of presentation [8]. The clinical findings previously described of appendicular endometriosis are acute and chronic appendicitis [2, 6, 9], intestinal intussusception and occlusion [4], perforated acute appendicitis [9, 10] and finally our case with the hemoperitoneum as a complication of acute appendicitis caused by endometriosis, where after laparoscopic diagnosis and treatment, the histological result obtained confirmed the etiology, besides clinical improvement and good postoperative evolution of the patient.
Appendicular endometriosis is a rare cause of acute appendicitis, and just in a few cases minimal bleeding in the lamina propria has been described previously [8], being our case an example of possible moderate hemoperitoneum associated with this disease.
The appendix is not a common focus site for endometriosis with an incidence of just 0.8% described in the literature. A few cases of acute appendicitis due to this pathology have been reported; however, none of them associated with hemoperitoneum with no pelvic organs affected. As for any rare case we consider this clinical presentation a new data to bear in mind when making a differential diagnosis in fertile patients, who present a compatible clinical scenario.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}