





Abstract
A urinoma is a collection of urine outside the urinary tract as a result of disruption of the collecting system. Obstructive causes of urine extravasation secondary to stones are not unseen but display a delayed diagnosis due to the gradual onset of symptoms, which can mimic pyelonephritis. We present the case of a 70-year-old female patient who was admitted to hospital with symptoms of right loin pain and sepsis. We describe her case from the initial clinical diagnosis of pyelonephritis to the final diagnosis of an infected urinoma after a calyceal rupture from an obstructive partial staghorn calculus. This case highlights the importance of early computerized tomography imaging in patients with renal stones and suspected pyelonephritis as ultrasound scans can sometimes be misleading. Misdiagnosis of infected urinomas delays definitive treatment and leads to increased morbidity.
INTRODUCTION
Acute pyelonephritis is a common acute urological admission to hospital, but occasionally we encounter the presence of an infected urinoma as the cause of the patients' symptoms. These two conditions closely resemble, but a delay in the diagnosis of an infected urinoma leads to increased morbidity. Therefore, inpatient imaging of the upper tracts, usually ultrasound scan (USS), takes place early on admission. In this case, USS failed to diagnose a collection leading to a delay in the management of an infected urinoma. We believe this case has important learning points that can help guide clinicians on a pathway that can lead to the timely diagnosis of similar cases in the future.
CASE REPORT
A 70-year-old female was admitted to hospital with 1-week history of right-sided loin pain, associated with urinary frequency and offensive smelling urine. She was febrile with nausea and vomiting and had similar recurrent symptoms for several months, which usually settled with oral antibiotics. She was haemodynamically stable, and abdominal examination revealed a soft non-peritonitic abdomen but with right loin and suprapubic discomfort.
Other than hypertension, arthritis and a kidney stone, over 10 years ago she had no other significant medical history. She did not recall the management of her kidney stone at the time as it was managed in another hospital.
Urinalysis on admission was positive for blood and leukocytes, but subsequent urine culture failed to demonstrate any specific bacterial growth, possibly due to the fact that she had recently been on antibiotics. She had a raised white cell count (WCC) of 22.6 and C-reactive protein (CRP) of 158 on admission with normal renal function. An X-ray of her kidneys (XR-KUB) performed in the emergency department revealed a 2.7 cm partial staghorn stone in her right kidney likely occupying her lower pole calyx and possibly part of the renal pelvis (Fig. 1).

The XR-KUB showing a right lower pole staghorn calculus.
A clinical diagnosis of right pyelonephritis was made. After discussion with the microbiologists, we commenced empirical intravenous antibiotics (co-amoxiclav and gentamicin) in view of the absence of prior positive urine cultures.
An urgent USS confirmed a staghorn calculus in the lower pole of her right kidney and an apparent 66 mm simple cyst was also identified adjacent to the lower pole of the kidney (Fig. 2). There was no hydronephrosis seen in either the kidney and the bladder appeared to be normal as well.
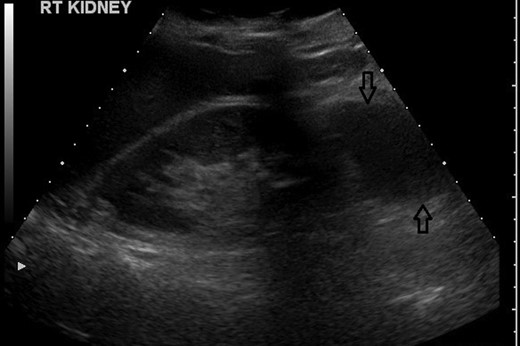
USS showing a suspected simple cyst on the lower pole of the right kidney.
Despite intravenous antibiotics, after 72 h, the patient reported ongoing right loin pain and with persistently raised WCC at 16.6. A decision was made to proceed with a computerized tomography (CT) scan. This showed a bi-limbed right lower pole staghorn calculus measuring 29 × 16 mm associated with a 53 × 56 × 33 mm fluid collection within the right perinephric space. This was associated with inflammatory stranding abutting the lower pole in keeping with a urinoma secondary to a ruptured lower pole calyx, which was not dilated at the time of the scan (Figs 3 and 4).

A non-contrast CT coronal view, showing the right kidney with a retroperitoneal collection associated with the lower pole. The stone is anterior to this CT slice.

A CT sagittal view, showing the calculus in the lower pole calyx and the collection below the kidney.
She had an USS-guided percutaneous drainage of this collection the same day and 45 ml of pus was drained. A pigtail drain was left in situ for 4 days, and as there was no hydronephrosis, we did not insert a ureteric stent or nephrostomy. She improved significantly after this event, and her inflammatory markers normalized. The pus culture showed a mixed organism growth.
She was discharged home with oral co-amoxiclav and as a renogram showed good drainage of her right kidney contributing 41% of her total renal function and she underwent a percutaneous nephrolithotomy (PCNL) from which she made an unremarkable recovery and returned to her normal activities.
DISCUSSION
A urinoma is a collection of urine outside the urinary tract as a result of disruption of the collecting system [1, 2]. Causes reported in the literature are blunt or penetrating renal trauma, after upper tract instrumentation, obstructive urinary tract stone, pelvico-ureteric junction obstruction and rarely cortical cyst rupture [1–8].
The majority of urinomas reported in the literature have a delayed diagnosis due to the gradual onset of symptoms, including loin pain and, when they become infected, sepsis [1, 6, 7]. Pain in the loin and infection are commonly thought to be the effects of pyelonephritis, and USS is an appropriate first-line investigation to exclude hydronephrosis or collections. USS though is operator dependent and does not provide reconstruction images or views of the whole upper tracts. CT offers non-operator-dependent imaging and also reconstruction images for percutaneous intervention and surgical access planning [5–8]. Cases of infected urinomas in the literature have the common initial diagnosis of a urinary tract infection up to the point of CT or magnetic resonance imaging (MRI) [1, 3, 8].
In our case, a CT scan was not performed on admission as there was no suggestive history of a ureteric calculus and USS suggested the presence of a simple cyst in the lower pole of her right kidney, a staghorn stone and no hydronephrosis. Persistent pain and raised inflammatory markers led to a CT scan, which revealed that the simple cyst reported in the USS was in fact a urinoma secondary to a ruptured lower pole calyx from a partial staghorn stone. This was confirmed with percutaneous drainage of pus from this area with resolution of the patients' pain and normalization of serum inflammatory markers.
It is, therefore, important that patients treated with intravenous antibiotics for suspected pyelonephritis secondary to staghorn calculi are closely monitored during their stay in hospital. CT imaging is a preferable method of investigation of these cases when they fail to respond to treatment.
CONFLICT OF INTEREST STATEMENT
We declare no conflict of interest. Informed consent was obtained from the patient for the use of anonymized images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}