





Abstract
A 72-year-old man presented with a 3-day history of recurrent transient ischaemic attacks comprising slurred speech, left arm weakness and paresthesia. Carotid Doppler revealed total occlusion of the right internal carotid artery (ICA). Computed tomography angiography demonstrated occlusion of the proximal right ICA over a length of 1.5 cm. The ICA distal to the occlusion was entirely normal. In view of the normal distal ICA, a decision was made to proceed with surgical exploration and right carotid endarterectomy, on the basis that there must have been some flow through the lesion. Intra-operatively, there was an extensive plaque in the carotid bulb and proximal ICA causing 80–90% stenosis. Fresh thrombus completed the occlusion. An aberrant branch of the ICA was identified distal to the plaque, the backflow through which maintained patency of the distal ICA. A standard endarterectomy was performed. The patient recovered uneventfully, being discharged on the second post-operative day.
INTRODUCTION
The common carotid artery (CCA) gives rise to the external carotid artery (ECA) and the internal carotid artery (ICA). The ICA is a terminal branch which does not give rise to any named branches in the neck. It divides into the anterior and middle cerebral arteries intracranially [1].
ICA occlusion can lead to potentially devastating ipsilateral cerebral infarct. The degree of cerebral ischaemia may vary depending on the collateral circulation from the ipsilateral vertebral artery or the contralateral vessels via the circle of Willis. Aberrant ICA branches are rare. Alternative ECA-to-ICA shunting via anomalous branches has been previously reported [2–4]. There have been just two cases of ICA branches distal to an occluded proximal ICA segment maintaining ICA patency in the literature [3, 5].
CASE REPORT
A 72-year-old man presented with a sudden onset of slurred speech, left upper limb weakness and paresthesia. During the subsequent 72 h, he had two similar episodes, each lasting for ∼4 min with complete resolution. He denied amaurosis fugax.
He was hypertensive, and medications included nebivolol, doxazocin, valsartan, pantoprazole and aspirin. He was a smoker of 20 cigarettes a day for 20 years.
Computed tomography (CT) of the brain revealed no acute abnormality. Carotid Doppler showed mild plaque in the left ICA and total occlusion of the right ICA. CT carotid angiography demonstrated total occlusion of the right proximal ICA over a length of 1.5 cm. The right ICA distal to the occluded segment was entirely normal.
If the entire right ICA was occluded, the patient would have been managed conservatively on best medical therapy. However, normal ICA distal to the apparently occluded segment suggested some flow through the plaque, or an anomalous distal branch.
A clinical decision was made to proceed with right carotid endarterectomy. Under general anaesthetic, a cervical incision was made parallel and anterior to the sternocleidomastoid muscle, centred over the carotid bifurcation. The CCA, ECA, superior thyroid artery and ICA were dissected and controlled. Vessels were inflamed with surrounding fibrosis. Carotid stump pressure was not measured due to proximal ICA occlusion suggested by CT angiography. There was an extensive plaque in the bulb and proximal ICA causing 80–90% stenosis, with fresh thrombus filling the narrowed portion. There was adequate pulsatile backflow from the distal ICA.
During dissection, an aberrant branch of the ICA was identified ∼2.5 cm distal to the bifurcation. Palpation and external examination of this branch revealed a soft artery without evidence of atherosclerotic disease. Immediately after the origin, this aberrant ICA branch coursed cranially, parallel to the ICA.
A standard endarterectomy was performed. The arteriotomy was closed primarily with 6/0 polypropylene. The patient made an uneventful recovery and was discharged on the second post-operative day.
Histology of the plaque revealed calcified atheromatous plaque with intra-luminal thrombus containing focal nuclear karyorrhexis and acute inflammatory cells.
DISCUSSION
We report a very rare case of an extracranial ICA branch preventing complete occlusion of the ICA distal to a heavily atherosclerotic occluded proximal segment. A normal ICA distal to the occluded segment raised the suspicion that some blood flow was maintained. Surgical exploration demonstrated an aberrant ICA branch ∼2.5 cm from the bifurcation. Carotid endarterectomy was successful and this prevented further transient ischaemic attacks and potentially devastating stroke. Pre-operative CT carotid angiography was reviewed retrospectively and this aberrant ICA branch was identified, albeit with a faintly visible origin (Fig. 1).
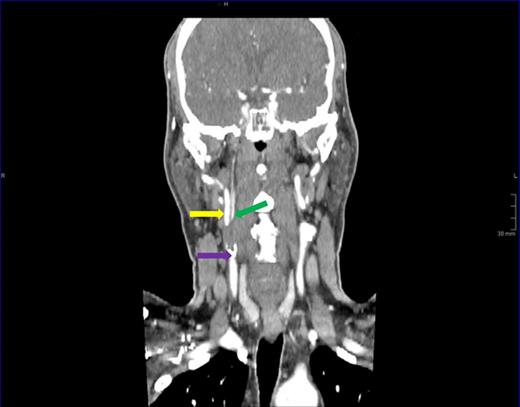
Sagittal plane view of the right carotid artery. Carotid bulb (purple arrow) gives rise to the internal carotid artery (yellow arrow) and an aberrant distal branch (green arrow).
Two previous cases with similar anatomical anomalies and clinical picture have been reported. Benson and Hamer, Jones and Simms described anomalous branches arising 2 cm from the carotid bifurcation preserving distal ICA flow [3–5]. Benson and Hamer demonstrated by angiography that this branch arose from the occipital artery [3].
Carotid imaging is still not perfect in distinguishing total from near total occlusion. The interpretation of contrast flow may be compromised by extensive calcified plaque. Several studies have emphasized the importance of determining patency of distal ICA as flow in the presence of an occluded proximal segment indicates anomalous collaterals which makes surgical exploration and endarterectomy feasible [5, 6].
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}