





Abstract
Femoral pseudoaneurysm is a common occurrence in intravenous drug abuser due to repeated trauma to the femoral artery causing arterial leak contained by the surrounding tissue and does not contain all the layers of arterial wall. Rupture of these aneurysm to exterior is a common presentation while rupture into surrounding structure deemed an emergency surgical attention. Hence, we report an unusual case of rupture of femoral pseudoaneurysm into urinary bladder who presented us with history of hematuria and was successfully managed.
INTRODUCTION
Femoral pseudoaneurysm are a common occurrence in intravenous (IV) drug abuser resulting from an arterial leak due to repeated trauma contained by the surrounding tissue without all layers of arterial wall presenting as a groin swelling [1]. These pseudoaneurysms need special attention to diagnose and intervene before they rupture [2]. Hematuria is a common presentation in urological patients but association of femoral pseudoaneurysm rupturing into urinary bladder and presenting as hematuria is a rare presentation. We did a search in MEDLINE, PubMed and Google and could not find any article reporting this uncommon association; hence, we present this case.
CASE REPORT
A 25-year-old HCV-positive male with a history of IV drug abuse for the past 3 years presented to our institution with complaint of pain lower abdomen and frank hematuria after receiving a minimal blow to his lower abdomen by his 4-year-old daughter during her play 6 days back. On arrival to our emergency room, the patient was conscious oriented tachycardic with a diffuse nonpainful nontender swelling in his right groin. Rest of his vitals and general examination was within normal limits. Distal pulsation in the right leg was present. His hemoglobin was 6.3 g% and CBC was high. Ultrasonogram of abdomen and pelvis revealed distended urinary bladder with clots and pseudoaneurysm of right common femoral artery measuring ∼112 × 69 × 87 mm (Fig. 1). The patient was planned for urinary bladder exploration along with evacuation of clot by urology team by cystoscopy after adequate resuscitation. During cystoscopy, nothing was visible due to massive clot inside the bladder which was incompletely evacuated so three-way Foley catheter was left in situ for continuous postoperative irrigation. Postoperatively, hematuria continued despite transfusion and, hence, emergent abdominal pelvic CT scan was performed.
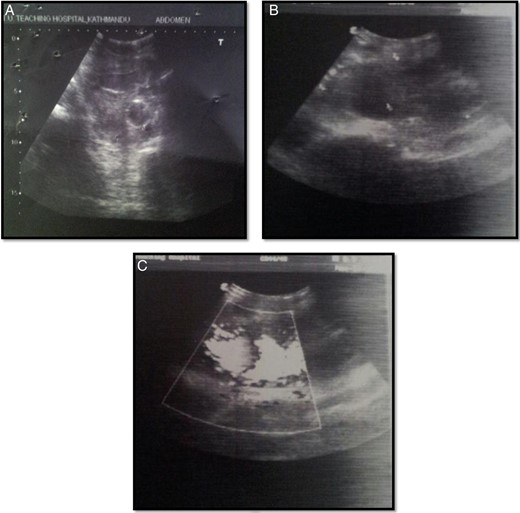
Arterial Doppler pictures: (A) urinary bladder with Foley's in situ and echogenic content likely clots; (B) large solid-cystic pulsatile lesion noted in the right inguinal region; (C) lesion in connection with common femoral artery via wide neck which showed to and fro spectral wave form (classical Ying Yang flow).
On contrast enhanced CT, a right common femoral pseudoaneurysm of size 12.5 × 6 × 6.5 cm was noted with intra-abdominal extension. Huge clot was also noted in the bladder with no obvious lesion in the kidney, ureter and bladder (Fig. 2). Thus, the patient was planned for exploration of pseudoaneurysm and urinary bladder. On exploration of right groin, there was a huge pseudoaneurysm in the groin extending above the inguinal ligament with 1 l of clot and blood (Fig. 3). Femoral artery was transected and proximal and distal ends were taken into control. Proximal end of femoral artery was ligated, and the leg was examined for distal saturation which was normal, so the distal end was also ligated. After addressing the femoral artery, the urinary bladder was explored. A small rent (∼0.5 × 0.5 cm) was noted in the right lateral wall of the bladder which was communicating with the wall of the pseudoaneurysm along with 2 l of blood and clot in the bladder. Thus, the enigma of hematuria was solved. Bladder was repaired according to standard technique and drain was kept in retroperitoneal space and abdomen was closed.
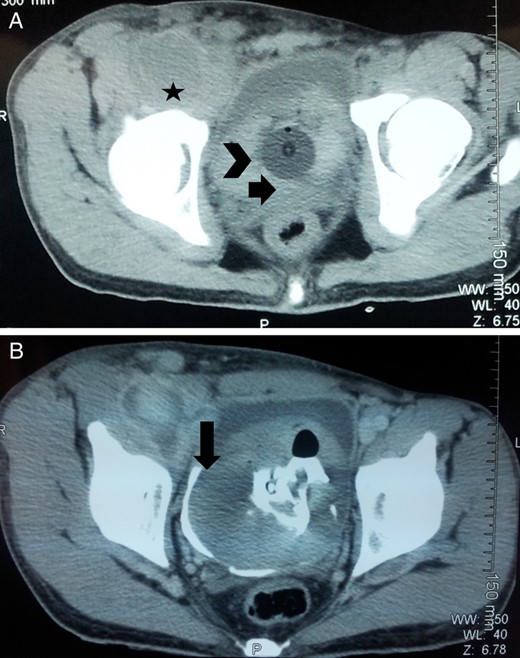
Axial CECT abdomen and pelvis pmages: (A) femoral pseudoaneurysm (marked with star), urinary bladder with clots (arrowhead) and Foley's catheter in situ (arrow); (B) communication between pseudoaneurysm and urinary bladder which was overlooked preoperatively (marked by arrow).
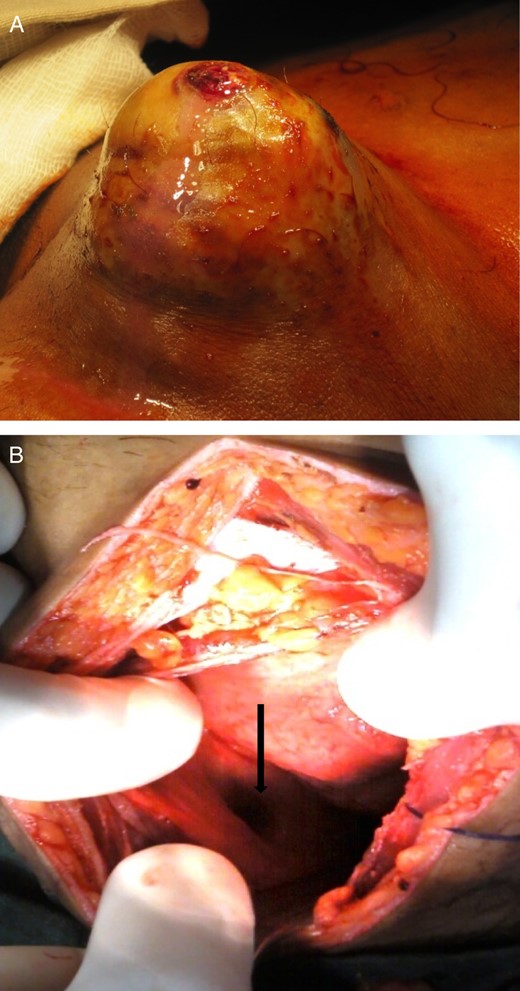
(A) Infected femoral pseudoaneurysm in an IV drug abuser; (B) intraoperative picture showing the communicating rent between pseudoaneurysm and bladder (marked by arrow).
Postoperatively, the patient had a speedy recovery and was discharged on the 7th postoperative day with Foley's catheter in situ. The distal limb is viable and the wound healing is satisfactory. Foley's catheter was removed after 2 weeks and the patient is doing well till date.
DISCUSSION
Hematuria is a common presentation of many urological problems, most commonly being urinary tract infection, urolithiasis and benign prostatic hyperplasia. Arteriovesical fistulas presenting as hematuria has been reported to occur after iatrogenic injury, secondary to trauma and spontaneously but a pseudoaneurysm rupturing into bladder is a rare presentation [3].
Rous et al. [4] reported the first case of a ruptured posttraumatic pseudoaneurysm of the external iliac artery 1 week after a gunshot wound to the lateral aspect of the bladder. To our knowledge, there have been 12 reported cases of arteriovesicular fistula (2 cases of spontaneous rupture, 3 cases post surgical, 4 cases post radiotherapy and 3 cases after urological intervention) [5]. When patients with vascular disease undergo pelvic surgery, radiotherapy or urological interventions, it weakens the wall of urinary tract and leads to arteriovesical fistulas. There are only two cases where an arteriovesical fistula formed spontaneously due to a ruptured iliac artery aneurysm with hematuria as initial presentation [6].
Femoral pseudoaneurysm, the most common arterial complication in IV drug abusers results from self-injection of drugs in the groin as it is easy and commonly assessable site. Repeated trauma to the vessel leads to formation of pseudoaneurysm which may presents as a painful pulsating mass, an infected mass or may even present with rupture [2]. Rupture of femoral pseudoaneurysm intramuscularly, intraperitoneally and retroperitoneally has been described but its communication with the bladder is extremely rare. It might be a coincidence that, in this case, the rupture of pseudoaneurysm provoked by recurrent puncture of femoral artery to administer IV drug and rupture of urinary bladder provoked by trivial trauma probably in full bladder, both occurred simultaneously.
The debate regarding reconstruction of infected pseudoaneurysm of the femoral bifurcation is of particular interest in this subset of patients [1, 7]. If the reconstruction requires a prosthetic material, then the resulting re-infection could be more complicated and dangerous. Therefore, from that point of view, most of the authors have advocated simple arterial ligation and resection of the infected tissues [8]. Ligation is the optimal management for infected pseudoaneurysms because it is easy, cost-effective and safe. Early reconstruction is not recommended when there is an extended infection in the area of the pseudoaneurysm. Moreover, infection of the artificial graft is also not uncommon. On the other hand, reconstruction of a vessel as at a first attempt can lead to development of aneurysms in the suture line. The arterial reconstruction may also be in jeopardy because of the IV drug abusers' tendency to reuse the femoral sites for further drug administration. Furthermore, the subcutaneous sites of extra-anatomical grafts increase their access for the reuse of the artery for injection and cause recurrent infection. Consequently, ligation is the optimal management of infected pseudoaneurysm in IV drug abusers [9]. Hence, in this case, we performed a simple ligation of proximal and distal end of the vessels, and it did not jeopardize the limb of the patient. Probably, multiple self-inflicted trauma in these patients lead to formation of collaterals supplying the distal limb which maintains the circulation even after ligation of the vessel.
Among various causes of hematuria, rupture of pseudoaneurysm into urinary bladder can be one of the rare causes especially in IV drug abuser which should be excluded with proper investigation before exploring the bladder. Infected femoral pseudoaneurysm in IV drug abusers can be effectively treated with simple debridement and ligation of the vessel without limb loss [9].
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}