





Abstract
Fournier's gangrene (FG) requires prompt recognition and management. We report the case of a 68-year-old man who presented with extensive pain and purple discolouration from the right iliac fossa to perineum. Computed tomography demonstrated gas within the right hemiscrotum extending into the inguinal canal and right buttock, with a right pelvic fluid and air collection. At debridement necrotic fluid was arising from the superficial inguinal ring so laparotomy was performed, revealing a grossly inflamed appendix herniating into the inguinal canal; a right hemicolectomy was performed. Unfortunately, the patient went into cardiac arrest and passed away on the operating table. Histological analysis demonstrated acute-on-chronic inflammation involving the appendix. The condition where appendicitis is implicated in FG is usually due to retroperitoneal rupture and tracking into the perineal spaces. This is the first case reported of an inflamed appendix herniating into the inguinal canal and thus causing FG.
INTRODUCTION
Fournier's gangrene (FG) is a very severe infection of the perineum and genitalia requiring prompt recognition and intervention. We report the very first case where it has been caused by an inflamed appendix entering the deep inguinal ring. Various intra-abdominal pathologies have been recognized as causes, but we believe this to be the first reported case.
CASE REPORT
A 68-year-old Caucasian man presented with a 3-day history of increasing right iliac fossa pain with swelling in the inguinal and scrotal regions, fever, rigors and malaise. He had a background of moderate systolic impairment, a left ventricular thrombus for which he was taking Warfarin, and asthma. He was not diabetic. He reported 3 days of right iliac fossa pain treated with analgesia.
On arrival to hospital, he was alert but haemodynamically collapsed. Systolic blood pressure rose to 60 mmHg with aggressive fluid resuscitation. On examination, there was extensive bruising in the right iliac fossa tracking into the inguinal region with a tender well-demarcated dark purple discolouration of the entire scrotum and perineal region. Surgical emphysema was present. Lower abdominal peritonism was demonstrable. FG was diagnosed.
Blood tests showed grossly elevated white cell count and acute kidney injury, along with markedly deranged clotting parameters (Table 1). The patient was resuscitated with further intravenous fluids, and broad-spectrum antibiotics were commenced. Prothrombin complex concentrate was administered to correct the international normalized ratio. En route to theatre for surgical debridement the patient underwent computed tomography (CT) to assess for intra-abdominal sepsis, given the clinical findings of lower abdominal peritonism and the recent reported lower abdominal pain. This revealed a large amount of loculated gas mainly within the right hemiscrotum with superior extension into the inguinal canal, lower anterior abdominal wall and subcutaneous soft tissue, and lateral extension towards the right buttock; along the right lateral pelvic wall, there was a 10 × 4 × 6 cm collection containing fluid and air. No bowel loops were identified extending into the inguinal region (Figs 1 and 2).
Blood results on admission.
| Haematology | |
| Haemoglobin | 13.2 g/dl |
| White cell count | 35.8 × 109/l |
| Platelet count | 495 × 109/l |
| Neutrophil count | 33.7 × 109/l (94%) |
| International normalized ratio | >20.0 |
| Biochemistry | |
| Sodium | 129 mmol/l |
| Potassium | 5.7 mmol/l |
| Urea | 23.6 mmol/l |
| Creatinine | 182 umol/l |
| Creatinine kinase | 443 u/l |
| Venous lactate | 5.7 mmol/l |
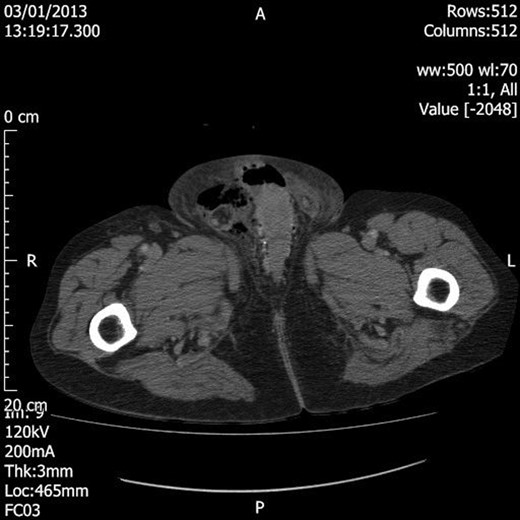
Axial section CT image demonstrating loculated air within the right hemiscrotum.

Coronal section CT image demonstrating extension of the loculated air superiorly into the inguinal canal and lower anterior abdominal wall and laterally into the right buttock. There is also a 10 × 4 × 6 cm fluid and air collection in the right pelvis.
Intra-operatively much of the scrotum and perineum was found to be devitalized and was therefore extensively debrided. Necrotic fluid was draining from the superficial inguinal ring; a decision was made to explore the abdomen, and laparotomy was performed. This revealed a grossly inflamed appendix herniating into the inguinal canal with an ischaemic caecum. A right hemicolectomy was performed. Unfortunately, the patient, who had remained haemodynamically unstable throughout the procedure, went into cardiac arrest. Despite five cycles of cardiopulmonary resuscitation he passed away on the operating table.
Subsequent histological analysis of the resected specimen demonstrated acute-on-chronic inflammation involving the appendiceal remnants and serosal surface, with serositis involving the caecum and inflammation focally extending into the caecal muscularis propria. The appendix itself lacked mucosa and showed acute-on-chronic inflammation with serositis. Anaerobic blood cultures taken at the time of admission subsequently grew Bacteroides fragilis.
DISCUSSION
Necrotizing fasciitis is a rapidly progressing soft tissue infection, usually caused by gas-forming anaerobic bacteria acting in a synergistic manner whereby there are arteritis and thrombosis of the small subcutaneous blood vessels, causing gangrene of the overlying skin and soft tissue [1]. FG is the term applied to the form of this disease affecting the perineum, perianal region and scrotum. It is named after the French dermatologist and venereologist Jean Alfred Fournier who in 1884 described five cases of young males affected by a rapidly progressing fulminant infection of the soft tissues in the perineal and scrotal regions, but there was no identifiable aetiology [2]. The most important risk factor is diabetes mellitus, and it affects males more commonly [3]. Although rare, FG has a high mortality rate reported to be as high as 67%, and so early recognition and management are vital [3].
The most common sources of infection identified in this condition have been from the urinary tract and perineal area with traumatic injury as another important cause [3]. However, more recently intra-abdominal pathologies have been reported as causes, mainly arising from the large bowel. While perforated diverticular disease and bowel malignancies have been described, acute appendicitis has been recognized as another cause of FG, mainly due to rupture of the viscus in the retrocaecal or retroperitoneal spaces with subsequent tracking of infection into the perineal and scrotal regions [4]. To our knowledge, this is the first reported case of FG where an inflamed appendix has been discovered to be herniating into the inguinal canal.
As mentioned earlier, early recognition and intervention are necessary to manage FG. Aggressive resuscitation of the patient with intravenous fluid therapy and broad-spectrum antibiotics is warranted together with initial blood tests and cultures to identify a causative organism. Unfortunately, the severity of the sepsis in this condition can cause a severe derangement in clotting parameters, as demonstrated in this case and potentiated by the patient taking Warfarin pre-admission. The need to stabilize the clotting parameter undoubtedly delays inevitable surgical debridement and is thus a major challenge in treating such cases.
The role of imaging in cases of FG has become more common recently, particularly with the increasing use and availability of CT scans in the emergency situation [5]. Although it could be argued that early surgical debridement takes priority, the use of CT scanning in the acute situation can aid not only in diagnosing FG with characteristic features such as subcutaneous emphysema and abscess formation but also in determining the source of gangrene, extent of the disease and routes of spread [5]. This of course requires very good knowledge of the relevant radiological features, but imaging is now being recognized as an increasingly useful tool in managing FG. In this case, inflammatory changes were recognized within the inguinal region, and this led to the extension of the original operation to a laparotomy where the source of the infection was discovered albeit with mortality as the outcome.
FG is a life-threatening surgical emergency, which can be caused by intra-abdominal processes, in this case an acutely inflamed appendix entering the deep inguinal ring. Pre-operative CT scan can aid in determining the extent of disease. Aggressive resuscitation and prompt surgical management remain the cornerstone of management.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}