





Abstract
Leiomyosarcomas are rare tumours of smooth muscle origin, and there have been no reported cases of such tumours arising within the ischiorectal fossa. Surgical resection with clear margins remains the gold standard treatment; however, there is limited literature on surgical approaches to the ischiorectal fossa for such tumours. We report a case of a high-grade leiomyosarcoma in a 59-year-old lady, occurring within the ischiorectal fossa that was managed using a novel simultaneous sphincter and sciatic nerve preserving trans-abdominal and trans-gluteal technique. This novel approach could be utilized not only for sarcomas but also for other tumours of the ischiorectal fossa extending into the gluteal region.
INTRODUCTION
Leiomyosarcomas are extremely uncommon in the rectum accounting only for 0.1% of all colorectal malignancies, and none has been reported to arise from within the ischiorectal fossa [1–3]. Surgical management with clear resection margins remains the gold standard treatment for sarcomas; however, the literature on surgical approaches to sarcomas within the ischiorectal fossa is limited. We report a case of a high-grade leiomyosarcoma occurring within the ischiorectal fossa that was managed using a novel simultaneous sphincter and sciatic nerve preserving trans-abdominal and trans-gluteal technique.
CASE REPORT
A 59-year-old lady presented with a 6-month history of a large, painless swelling in her right buttock with an associated change in bowel habit towards looser stools. On physical examination, there was a palpable, firm, fixed swelling of 4 × 3 cm in the right peri-anal region about 3 cm from the natal cleft. On digital rectal examination, the mass was palpable low down on the borders of the sacrum and coccyx. CT colonography showed a 9 cm × 5.6 cm × 4.5 cm lesion arising from the right medial aspect of her gluteus maximus, which displaced the mesorectal fascia and externally compressed the rectum. CT Pelvis showing a bilobed mass on the right side lying in the ischiorectal fossa extending out through the greater sciatic notch into the buttock measuring 9 cm × 6 cm × 4.5 cm (Fig. 1A and B).
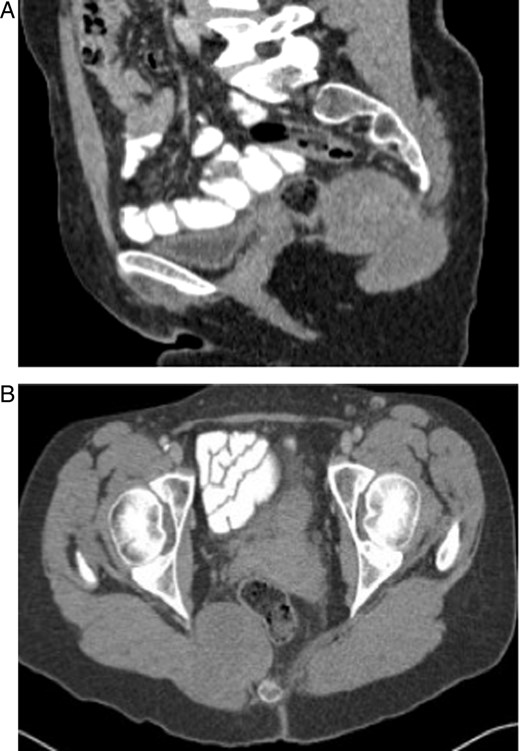
(A and B) CT scans of the tumour showing a bilobed mass within the ischiorectal fossa extending through the greater sciatic notch.
Ultrasound-guided biopsy of the tumour tissue confirmed a Grade 3 leiomyosarcoma with sheets of spindle cells with marked nuclear pleomorphism and a brightly eosinophilic cytoplasm. Immunocytochemical labelling was strongly positive for smooth muscle actin and desmin. A staging CT scan showed several small (<5 mm) indeterminate lesions in the liver and lung bases. Following a combined sarcoma/colorectal multi-disciplinary team (MDT) discussion, a joint excision of the ischiorectal leiomyosarcoma with simultaneous trans-abdominal and posterior trans-gluteal approach was planned.
The patient was placed in the left lateral position with a 45-degree tilt. Two surgical teams simultaneously performed the surgery. A colorectal surgeon was operating from the left side and a sarcoma surgeon was operating from the right side kneeling down for the duration of the operation lasting about 3 hours.
The tumour was firmly adherent to the anterior aspect of the sacrum and ischial spine. Fibres of the gluteus maximus were divided around the tumour, which was then mobilized from the midline attachment to the sacrum and coccyx. Meanwhile, the colorectal team approached the tumour from the peritoneum. The rectum was found to be non-adherent to the tumour and was dissected free of the rectum and the sphincter swept away. Almost two-thirds of the tumour was free apart from its attachment to the ischial spine and rectum. At this point, it was decided to carry out an intra-abdominal osteotomy of the distal sacrum to free the tumour. Four units of blood and fresh frozen plasma were required. The tumour was completely mobilized, the sacrospinous ligaments and parts of the ischial spine were divided and the tumour was delivered out through the gluteal wound. The sciatic nerve and anal sphincter were preserved. The peritoneal defect was repaired, and the wounds were closed using 1/0 and 2/0 vicryl and skin clips. A drain was placed in situ.
A pathological examination of the specimen confirmed a high-grade leiomyosarcoma with a maximum diameter of 80 mm and close but clear resection margins (R0) (Fig. 2). Microscopically, the tumour invaded skeletal muscle, had a thin pseudocapsule and was composed of sheets and broad interweaving fascicles of spindle cells demonstrating marked nuclear pleomorphism. There were significant oedema, fibrosis and necrosis with foci of vascular invasion.
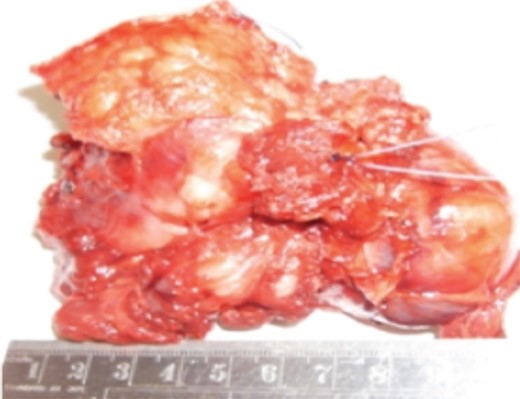
Pathological specimen.
The patient had full control of the anal sphincter, and there was no distal neurovascular deficit. The patient had no immediate or early complications from the procedure, and the wounds healed well. There was no evidence of local recurrence at 2-year follow-up. However, she developed multiple liver and lung metastases after 2 years. Following MDT discussion, it was decided to start chemotherapy with doxorubicin. Subsequently, she developed L2 spinal metastases, received palliative radiotherapy and commenced on trabectedin chemotherapy. The patient passed away 3 months later due to multiple metastases, 27 months after the surgical resection. However, she retained full anal sphincter control and sciatic nerve function till the end.
DISCUSSION
Peri-anal leiomyosarcomas are rare, and to our knowledge, there are no reported cases of leiomyosarcomas in the ischiorectal fossa [2, 3].
The first reported case of a sarcoma in the ischiorectal fossa was in 1988 by Long Pretz et al. of a liposarcoma [4]. Since then, only a handful of cases have been reported, with the second case not published until 2003 of an angiomyofibrosarcoma [5]. Other reported sarcomas include a malignant peripheral nerve sheath tumour (MPNST) [6] and a spindle cell sarcoma [7]. A variety of different operative techniques have been described to excise ischiorectal sarcomas, and the approach varies depending on the location, size and histology [7].
The combined trans-abdominal and trans-gluteal surgical approach provided the exposure required to dissect and remove the sarcoma from a difficult location. Osteotomy of the distal sacrum was performed safely as the proximal extent of the tumour was visible through the abdominal wound. The simultaneous approach facilitated safe complete resection of the sarcoma with preservation of the vital structures. This approach also has the potential to reduce the operating time. To perform the surgery, one of the surgeons undertaking the gluteal approach had to kneel down for about 3 hours. The other option would be to perform a sequential procedure—trans-abdominal mobilization of the tumour followed by trans-gluteal resection—this could result in a longer operation, increased blood loss and poor control of osteotomies if required.
We have presented the first reported case of a leiomyosarcoma removed from the ischiorectal fossa, using a simultaneous trans-gluteal and trans-abdominal approach that allowed R0 resection while preserving the anal sphincter and the sciatic nerve. This approach could be utilized not only for sarcomas but also for other tumours of the ischiorectal fossa extending into the gluteal region.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}