





Abstract
Klippel–Trenaunay syndrome (KTS) is a rare congenital disorder characterized by the triad of capillary malformations, atypical venous malformations and varicosities and bony and/or soft tissue hypertrophy. We present the case of an 18-year-old man with KTS affected by haematochezia secondary to rectal venous malformations that was managed with endoscopic sclerotherapy. In this case, we compared the use of ethanol to phenol as a sclerosant.
INTRODUCTION
Klippel–Trenaunay syndrome (KTS) is a rare congenital malformation first described in 1900 by Maurice Klippel and Paul Trenaunay. KTS is characterized by the triad of capillary malformations, atypical venous malformations and varicosities, and bony and/or soft tissue hypertrophy [1]. KTS is estimated to affect 1 in 100 000 people worldwide with no predilection to race or sex [2].
CASE REPORT
An 18-year-old man presented for consideration of exenteration of the rectum and giant venous malformations extending out the sciatic notch. He had experienced multiple significant episodes of haematochezia with associated anaemia (haemoglobin of 4.5 g/dl) and lethargy. This is on a background of KTS complicated by a right leg amputation, bleeding skin lesions and chronic haematochezia. A colonoscopy was performed that revealed a number of colonic vascular malformations. A non-obstructive pedunculated malformation was present near the ileocaecal valve occupying ∼50% of the lumen with the majority of malformations present in the rectum as a diffuse-dilated venous plexus (Fig. 1). A ‘N-of-1’ random allocation was performed to inject the rectum with 5 ml of phenol in almond oil to the left and 20 ml of 75% ethanol to the right-sided vessels just beyond the anorectal junction [4]. The patient returned at 6 months for a flexible sigmoidoscopy to assess the rectal venous malformations. At the time of presentation, there was no further history of haematochezia. The flexible sigmoidoscopy again identified the previous venous malformations with an obvious but subjective reduction in the right-sided lesions (ethanol-injected lesions) more so than the left (Fig. 2). A further 20 ml of 75% ethanol was injected into the left-sided lesions as well as 10 ml of 75% ethanol into the right-sided lesions. To date the patient has not reported any further haematochezia.

Pre-ethanol rectal venous malformations.
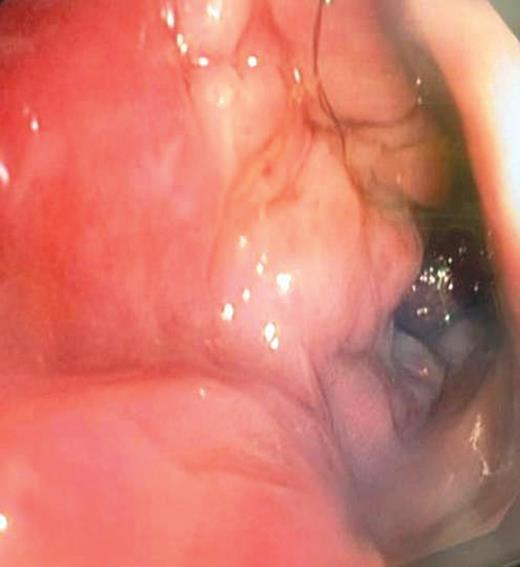
Six-month post-ethanol rectal venous malformations.
DISCUSSION
The rate of venous malformations in patients with KTS is ∼70% [1]. However, case studies suggest that the rate of problematic haematochezia associated with KTS is quite low [1, 3]. The severity and degree of haematochezia determines the choice of management in these individuals. Surgical management of rectal haemangiomas is dependent on the extent of the anatomy of the haemangioma. Proctocolectomy with coloanal anastomosis is an option that allows for preserved anal function with control of bleeding [5]. However, extension of the haemangioma to the perianal and perineal region may require abdominoperineal resection with a permanent colostomy [5]. An alternative management option is endoscopic sclerotherapy. Parashette and Cuffari describe the case of a child with KTS complicated by haematochezia where endoscopic sclerotherapy with 75% ethanol was successful [6]. Ethanol has been used in sclerotherapy for many years and is tolerated in most cases. However, systemic toxic side-effects of ethanol have been reported in the literature. Minor side-effects of percutaneous ethanol include skin blistering, ulceration and scar formation, while major side-effects include pulmonary embolism, cardiovascular collapse and death [7]. Wong et al. [7] have described cardiovascular collapse in the case of an 11-year-old child with KTS that underwent ethanol sclerotherapy. Yakes and Baker have described desaturation, bradycardia and cardiopulmonary collapse in three adults who underwent ethanol sclerotherapy [8]. Retrospective study has suggested that the only factor significantly associated with a systemic adverse event is the ethanol dose/weight ratio per intervention [9]. Bisdorff et al. [9] suggest a maximal ethanol dose/weight ratio of 0.2 ml/kg in the treatment of venous malformations with ethanol as a sclerosant.
This case offers further support for 75% ethanol as a sclerosant in the management of rectal venous malformations and their use in an adult population. It is important to note that the options for treatment of rectal venous malformations include surgery and/or endoscopic sclerotherapy, and that each of these options is associated with its own complications. Evidence does not exist in support of one mode of therapy over the other and the treatment option should be based on an individual assessment.

{kind=link}
{kind=link}