





Abstract
Intercostal incisional hernias are rarely encountered post-operative complications. Bone sequestra of the ribs are similarly rare. We report a very rare case of a left sided rib bone sequestrum mimicking an incisional hernia after a nephrectomy, splenectomy, and distal pancreatectomy.
INTRODUCTION
A bone sequestrum is devitalized, dead bone, typically resulting from necrosis secondary to trauma-related ischemia or following an infection, such as osteomyelitis [1]. Sequestra of the ribs have rarely been documented, with most appearing from tuberculosis infections [2]. Furthermore, intercostal incisional hernias are rare as well, with few etiologies [3, 4]. This is, to the best of our knowledge, the first report of a large rib sequestrum causing a bulge near a prior surgical scar site, leading to a preoperative diagnosis of an incisional hernia. Possible etiologies are discussed.
CASE REPORT
A 65-year-old female presented with a chief concern of left abdominal wall pain and possible incisional hernia. She had undergone a left radical nephrectomy, splenectomy and distal pancreatectomy earlier in the year for a mass on the left kidney. Pathologic evaluation revealed the mass to be a large perinephric abscess of uncertain etiology. Her recovery was complicated by a wound infection and development of a pancreatic fistula, which was repaired. A few months later, after recovery, the patient began experiencing significant pain at the incision site, which was worse with daily activity. She denied any symptoms of infection, such as fever or chills. A complete blood count performed shortly after surgery revealed no leuckocytosis. She was referred to general surgery for a suspected incisional hernia. Physical examination revealed a firm bulge at the superior aspect of the incision in the left upper quadrant, which was tender to palpation and non-reducible. There was no erythema, fluctuance or other signs of infection. An abdominal computed tomography (CT) scan revealed muscular laxity and a questionable abdominal wall hernia at the incision site (Fig. 1). The patient was taken to the operating room for abdominal wall wound exploration and possible hernia repair. The superior aspect of the previous incisional scar was reopened and dissection carried down through the subcutaneous tissue to the level of the fascia. No fascial defect was found; however, a firm mass was palpated within the abdominal wall. Further dissection revealed a malpositioned left rib surrounded by fibrous tissue. The rib appeared devitalized, thin and fragile. We then referred back to the CT scan and in this location, no calcification could be observed. However, this was clearly a rib. The rib was dissected until a healthy portion was noted and the devitalized rib was resected (Fig. 2). The wound was surveyed again for any muscular or fascial defects, none were found. The patient was discharged in good condition the same day. Removal of the rib sequestrum resolved the patient's symptoms.
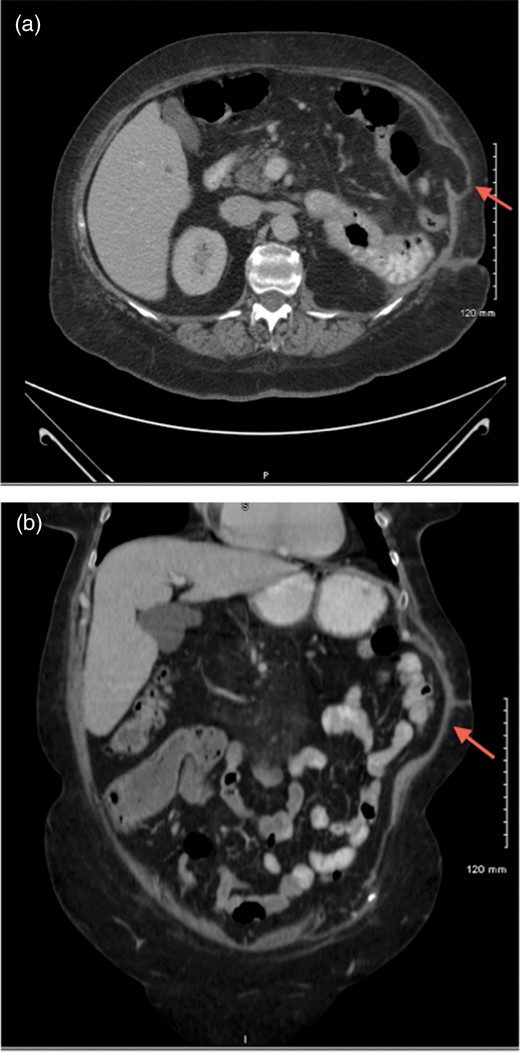
CT scans of abdomen showing a potential abdominal wall hernia (arrows).

Resected rib.
DISCUSSION
A bone sequestrum is devitalized or dead bone [1]. Infection, such as osteomyelitis, can lead to necrosis and form bone sequestra. There are many documented cases of osteomyelitis causing bone sequestra; however, sequestra of the ribs are rare, most of which are found to occur in patients with tuberculosis [2, 5, 6]. Trauma, leading to vascular compromise and ischemic injury, is a cause of dead bone as well [1]. Most rib sequestra reported in the medical literature resulted from an infectious etiology.
A reasonable explanation for this patient's rib sequestration is from an infectious source, such as osteomyelitis, which can be acute, sub-acute or chronic. Osteomyelitis is caused by a hematogenous source, trauma or direct inoculation via surgical or contiguous spread [5, 6]. With the patient's history of recent surgery for perinephric abscess and pancreatic fistula within the past year, both of these could lead to the seeding of an infection of her rib. Such an infection could trigger necrosis of bone and formation of her rib sequestrum. Due to the lack of symptoms other than pain, chronic osteomyelitis would be the most likely infection.
Trauma during her previous nephrectomy/splenectomy/pancreatectomy could have also contributed to a rib sequestrum. This long, major surgery would require much retracting force on the ribs and upon the tissue adjacent to them. This could lead to vascular compromise and ischemic injury leading to necrosis and sequestrum formation. As stated in the case, the rib was found to be malpositioned, supporting this etiology.
In either case, or by a combination of infection and ischemia, the rib sequestrum presented a diagnostic conundrum and interesting intra-operative findings. A high index of suspicion is necessary to diagnose and properly manage rib sequestrum.

{kind=link}
{kind=link}
{kind=link}
{kind=link}