





Abstract
Perilunate dislocations are a devastating injury to the carpus that carry a guarded long-term prognosis. Mayfield type 4 perilunate dislocations are rare, high-energy injuries that carry a risk for avascular necrosis (AVN) of the lunate. When AVN ensues and the carpus collapses, primary treatment with a proximal row carpectomy or arthrodesis has been advocated. This case reports a successful clinical result and revascularization of an extruded lunate with open reduction and internal fixation. This type 4, Gustilo grade 1 open perilunate dislocation exhibited complete avulsion of all lunate ligamentous attachments. Management included open reduction and internal fixation as well as carpal tunnel release through a combined dorsal and volar approach. Despite concerns for lunate AVN due to complete disruption of lunate vascularity, a 10-month postoperative clinical and radiographic examination demonstrated no pain with activities of daily living as well as a revascularized lunate.
INTRODUCTION
Perilunate dislocations are high-energy injuries primarily observed in younger individuals. The mechanism of injury consists of wrist hyperextension with ulnar deviation. Mayfield described a widely used classification system, where a type 4 injury consists of a lunate dislocation [1]. Due to the rarity of this injury, only a few reports including treatment outcomes exist in the literature [2–5]. While open reduction internal fixation (ORIF) is the treatment for types 1–3, treatment for type 4 is more controversial [2–5]. Lunate dislocation results in a disrupted vasculature, leading to an increased rate of AVN [3, 5]. The lunate receives its vascularity through dorsal and volar vessels. Previous reports of perilunate dislocations demonstrated a low rate of lunate AVN if the vascularity remains intact through volar ligamentous attachments [6, 7]. Despite these reports, continued concern for lunate AVN and carpal collapse has led some authors to advocate for proximal row carpectomy (PRC) or arthrodesis as the initial surgical treatment of type 4 injuries [3–5]. We report a grade 1 open, Mayfield type 4 perilunate dislocation with a devascularized lunate treated primarily with ORIF. To the authors' knowledge, this is the first report documenting an open perilunate dislocation with the lunate extruded from the carpus lacking any ligamentous attachments. There is a paucity of literature describing the management of type 4 perilunate dislocations. We report a successful outcome with revascularization of the lunate after a complete vascular disruption.
CASE REPORT
A 40-year-old male presented after a fall from two stories. Although the history and physical examination were limited secondary to intoxication and decreased Glasgow Coma Scale score, a deformity of the right wrist was observed. Physical and radiographic examination demonstrated an open, lunate enucleation with a 1.0 × 0.5 cm volar wound that communicated with bone (Fig. 1). Concern for subluxation of the second and third carpometacarpal joints (CMC) was also appreciated. However, a review of the patient's medical history demonstrated chronic CMC injuries to the right hand. Vascular examination was intact; however, a proper neurological examination was unobtainable due to the patient's obtunded condition. Initial management consisted of bedside washout, immobilization, tetanus prophylaxis and intravenous cefazolin. Further workup was negative and the patient was transferred emergently to the intensive care unit.
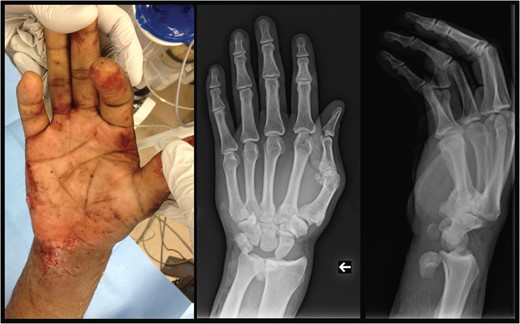
Left: preoperative gross depiction of injury. Center: antero-posterior view of the right wrist, demonstrating displacement of the lunate to a position just radial to the ulna. Right: lateral view of the right wrist, demonstrating displacement of the lunate anterior to the ulna/radius. Carpometacarpal subluxation is also noticed.
After stabilization, open reduction of the perilunate dislocation with a carpal tunnel release was performed through a combined volar and dorsal approach 12 h after presentation (Fig. 2). The lunate had no ligamentous attachments and was free floating in the distal forearm. The scapholunate and lunotriquetral ligaments were completely avulsed and irreparable. Reduction was achieved with manipulation using a joystick technique with K-wires placed into the scaphoid and lunate. K-wires were placed through the scaphocapitate, scapholunate and lunotriquetral intervals (Fig. 3). The CMC subluxations were stable when stressed under fluoroscopy, establishing the chronicity of these injuries.
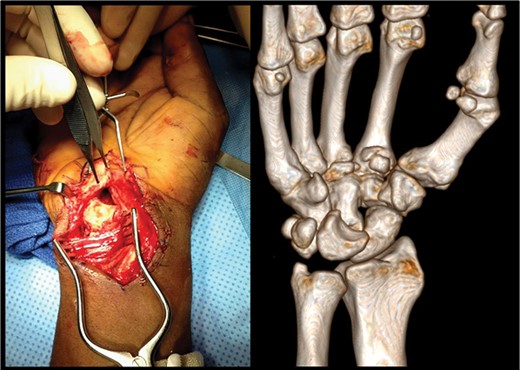
Left: intraoperative image demonstrating the dislocated lunate sitting anterior to the carpal tunnel prior to operative reduction. Right: preoperative volar view of a three-dimensional CT reconstruction of a right wrist. Dislocation of the lunate from the carpus is noted.
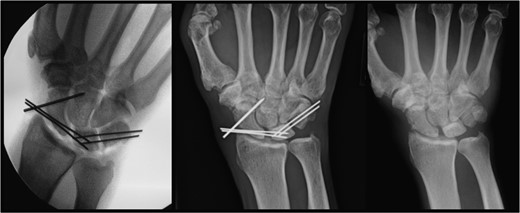
Left: intraoperative image demonstrating K-wires supporting the lunate. Center: postoperative image at 10 months demonstrating the lunate still in proper position with retained hardware. Right: postoperative image at 10 months demonstrating proper positioning of the lunate after removal of hardware.
Postoperative examination revealed a neurovascularly intact right upper extremity. The patient was lost to follow-up until presenting with symptomatic instrumentation 10 months postoperatively. Normal lunate radiographic density on X-rays confirmed revascularization of the lunate (Fig. 3). Clinical evaluation demonstrated a neurovascularly intact, stable carpus without evidence of carpal collapse or arthrosis (Fig. 3). The instrumentation was removed and the patient reported no pain with daily activities and full range of motion when compared with the uninjured left hand.
DISCUSSION
Perilunate fracture dislocations are the result of high-energy injuries to the carpus. In type IV perilunate dislocations with lunate extrusion, no standardized treatment exists. While the literature documents several closed lunate enucleations, the treatment for these injuries varied and included arthrodesis, PRC or ORIF with Kirschner wires (K-wires) [2–5]. The open injury and the complete avascular condition of the lunate distinguish this case from other type IV perilunate dislocations reported in the literature. Although previous reports have advocated for arthrodesis or PRC due to concern over lunate AVN and carpal collapse, ORIF at the index operation should be considered. As most injuries occur in younger, active patients, avoiding a PRC can help preserve carpal kinematics and grip strength. Chim demonstrated that a PRC exhibits a higher failure rate in younger populations or those involved in manual labor [8]. In a younger population presenting with lunate enucleation, achieving reduction and lunate revascularization with an open approach may prevent the sequelae of a PRC.
The lunate in type IV injuries commonly maintains vascularity through the tethered volar radiocarpal ligaments. In the rare case of complete ligamentous avulsion, vascularity is completely disrupted and a high suspicion for lunate AVN must be maintained. Despite total lunate vascular compromise in this patient, a 10-month radiographic follow-up demonstrated lunate revascularization and a stable carpus. While a previous report demonstrated that the lunate can survive a transient vascular compromise, it is difficult to explain how the lunate can revascularize just by its replacement into the carpus [9]. Ekerot hypothesized that lunate revascularization in a trans-scaphoid perilunate dislocation may occur through a united scaphoid fracture with an intact scapholunate ligament [7]. While this theory does make anatomical sense, our patient had a complete disruption of all ligamentous attachments. Emami et al. reported a similar patient with an extruded lunate and proximal pole of the scaphoid fracture that also retained no vascular attachments. They elected for ORIF, but lunate AVN subsequently developed [10]. When lunate extrusion is encountered, abstaining from a closed reduction attempt may help preserve any remaining vascular radiocarpal ligamentous attachments and decrease trauma to the median nerve.
Lunate extrusion into the carpal tunnel must be managed emergently. The open nature of this injury warranted an emergent operative washout and exploration. Advocating for ORIF in the setting of a type IV perilunate dislocation with lunate extrusion avoids the long-term sequelae or physical limitations of a PRC or arthrodesis in the younger patient population. In the event that the patient develops lunate AVN after ORIF, a PRC or arthrodesis may still be performed as a salvage operation. This case highlights the ability of the carpus to heal high-energy injuries involving open perilunate dislocations with a devascularized lunate. Emergent ORIF for open, type 4 perilunate injuries with an enucleated, devascularized lunate can still result in acceptable wrist function and lunate revascularization.
CONFLICTS OF INTEREST
None of the above authors have any conflicts of interest to disclose in the submission of this manuscript.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}