





Abstract
We report the case of a 78-year-old female who was found to have a mycotic thoracic aortic arch aneurysm caused by Clostridium septicum. Subsequent investigations demonstrated adenocarcinoma of the caecum with two liver metastases. The patient underwent a hybrid procedure involving endovascular repair of the aneurysm with a right-to-left carotid crossover bypass and a left carotid to left subclavian bypass to protect the cerebral and left subclavian blood flow. The caecal tumour was later completely excised by laparoscopic right hemicolectomy. The patient then underwent resection for the liver metastases. There was no evidence of tumour recurrence 2 years after her right hemicolectomy. This case emphasizes the importance of the association of C. septicum infection with colorectal malignancy. To our knowledge, this is the first case of a mycotic aortic arch aneurysm caused by C. septicum being successfully treated with a hybrid endovascular repair procedure.
INTRODUCTION
Clostridium septicum is a rod-shaped, gram-positive, flagellated bacterium. It is a member of the normal gut flora in humans as well as other animals. Septicaemia due to C. septicum can occur from trauma, surgery, skin infections/burns and obstetric infections. Gas gangrene is the commonest reported complication of C. septicum [1]. Clostridium septicum has a very strong association with malignancy, particularly colonic cancers [2]. Other bacterial infections that have been shown to be strongly associated with colorectal cancer are Streptococcus bovis, and to a lesser extent Bacteroides fragilis and Escherichia coli [3]
Mycotic aneurysms account for 2.6% of aortic aneurysms [4] and develop as a result of bacterial infection in the aortic wall. Salmonella species and Staphylococcus aureus are the most commonly isolated causative organisms. Mycotic aortic aneurysms associated with C. septicum infection are extremely rare with <30 cases currently reported in the literature.
Without surgical intervention, mycotic aortic aneurysms usually lead to uncontrolled sepsis or catastrophic haemorrhage [5]. The mortality associated with mycotic aortic aneurysms has been documented between 23 and 60% [6].
CASE REPORT
We report the case of a 78-year-old female who was admitted as an emergency with chest pain 9 days after shoulder arthroplasty.
Computed tomography (CT) pulmonary angiogram was performed to exclude pulmonary embolus, but demonstrated a 2-cm mycotic thoracic aortic aneurysm. The patient was commenced on intravenous meropenem and metronidazole as per microbiology advice. Blood cultures taken grew C. septicum, which is known to be associated with colonic malignancies [2]; therefore, a CT of the abdomen and pelvis was performed which showed localized thickening of the ascending colon at the level of the ileocaecal valve suspicious of large bowel malignancy, with two hepatic metastases consistent with T2N0M1 cancer of the caecum. Subsequent colonoscopy identified an ileocaecal tumour and biopsies confirmed moderately differentiated adenocarcinoma.
The patient remained on IV antibiotics while treatment was planned. An interval CT was performed 42 days after her initial diagnosis which showed that the aneurysm had significantly increased in size measuring up to 5.5 cm (Fig. 1 ).
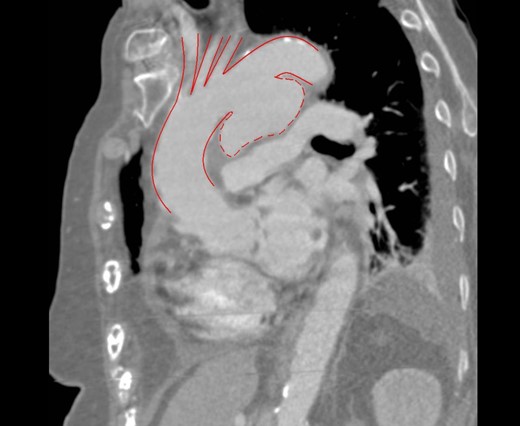
CT scan of the thorax demonstrating large mycotic aneurysm.
The decision was made to perform a hybrid procedure involving endovascular repair of the aneurysm and extra-anatomical bypass of the supra-aortic vessels with a right-to-left common carotid crossover bypass and a left common carotid to left subclavian bypass to protect the cerebral and left subclavian blood flow (Fig. 2). This was performed 46 days after admission. The patient was admitted to the ICU for 24 h post procedure and discharged from the hospital on the 25th postoperative day.

3D reconstructed CT scan showing the endovascular aortic arch repair.
Surveillance of the aneurysm repair showed persistent graft infection and an endoleak, so treatment for her caecal tumour was postponed while the patient underwent long-term antibiotic therapy. Repeat surveillance CT of her thorax, abdomen and pelvis 11 months later showed no significant clinical progression of her malignant disease.
Laparoscopic right hemicolectomy was performed 16 months after her aneurysm repair, and the patient was discharged home on the third postoperative day with no major complications. Histology showed Dukes' B cancer with no lymph node involvement and complete excision.
The patient underwent surgery for the liver metastases and had two segmental resections (segments III and V + cholecystectomy) 4 months after laparoscopic right hemicolectomy. Postoperative recovery was again uneventful and the patient was discharged on the 16th postoperative day. There was no evidence of recurrence on CT at 22 months, or on plasma carcinoembryonic antigen levels at 28 months after right hemicolectomy.
DISCUSSION
This case emphasizes the importance of the association of C. septicum infection with colorectal malignancy. A case series by Takano et al. [7] showed that, in patients with mycotic aortic aneurysms due to C. septicum, 14 of 19 cases had colonic neoplasms; of which, 11 were primary colonic tumours. Isolation of this pathogen therefore should always prompt clinicians to image the gastrointestinal tract with either CT or endoscopy to exclude occult malignancy. The same can also be said for isolation of S. bovis [3].
Endovascular repair of aortic aneurysms is an increasingly favourable approach compared with open repair. The challenge faced with the repair of aortic arch aneurysms is the involvement of the supra-aortic vessels (the braciocephalic, left carotid and left subclavian arteries) that can be occluded by the endovascular graft and result in stroke and limb ischaemia. This problem can be overcome using a hybrid approach that combines the endovascular repair with rerouting of the supra-aortic vessels.
The advent of hybrid treatment of the aortic arch provides an appealing option for high-risk patients who are unsuitable for open repairs as it eliminates the need for extensive arch and thoracic aorta dissection and the reduced time of total circulatory arrest [8].
Double transposition can be performed for aneurysms involving both the left subclavian and left common carotid vessels as in this case. This was first described in 2002 [9] and involved the anastomosis of the left common carotid artery to the brachiocephalic artery and anastomosis of the left subclavian artery to the already transposed left common carotid artery. Similar procedures have since been safely performed using prosthetic grafts, and right-to-left carotid crossover bypass which precludes the need for median sternotomy and provides acceptable stroke-free survival [10]. In the same study by Takano et al. [7], only 3 of the 19 cases involved the aortic arch and 2 of these 3 cases died (1 from cardiac tamponade and 1 from presumed sepsis) and 1 case survived after open surgery (although the aneurysm did not involve the supra-aortic vessels). To our knowledge, this is the first reported case of a mycotic aneurysm of the aortic arch caused by C. septicum that has been successfully treated with a hybrid technique endovascular repair.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}