





Abstract
Popliteal soft tissue sarcoma is a rare tumour, but sometimes it does pose clinical, diagnostic and management challenges. We present here a case report which initially presented as Baker's cyst as it is one of the commonest cyst in this region. It posed a diagnostic challenge even with the help of new imaging modalities. But the patient presented herself to the hospital several times with new symptoms often pointing us towards common pathologies like Baker's cyst, deep-vein thrombosis and vascular lesions but diagnosis was established only after histology. Unfortunately, at this stage, disease was so advanced and metastasised, patient reached terminal stage and refused any kind of treatment.
INTRODUCTION
Baker’s cysts are enlargements of gastrocnemius-semimembranosus bursa that lies between these muscles on the medial side of the popliteal fossa, slightly distal to the center crease of the knee [1]. Twenty-six percent of cysts were found in patients 31–50 years, whereas 53% were found in ages 51–90 years [2]. Most common conditions associated with Baker's cyst are osteoarthritis, rheumatoid arthritis and Juvenile rheumatoid arthritis. However, it is important to exclude other differential diagnoses such as lipoma, aneurysm and soft tissue tumour. The latter can have catastrophic outcome for the patient if diagnosis is delayed.
CASE REPORT
An 80-year-old female presented to the general practitioner with 3-month-old history of gradual onset swelling in the back of her right knee, painful right leg and swelling in her right ankle. There was no history of trauma, constitutional symptoms, weight loss or loss of appetite. She lived alone and was independently mobile.
She suffered from gout, hypertension and asthma but otherwise quite fit for her age.
On examination, she had a nontender 5 × 5 cm fluctuant and nonpulsatile lump in popliteal fossa with no overlying skin changes.
An ultrasound scan (Fig. 1) revealed a large mass lesion with heterogeneous appearances in the popliteal fossa extending between the two heads of the gastronemii and large blood vessels in the central region of the mass. It measured ∼13 × 5.5 × 4.5 cm in dimension and a magnetic resonance imaging (MRI) scan was suggested to rule out mass arising from the popliteal vessels being enveloped by the mass.
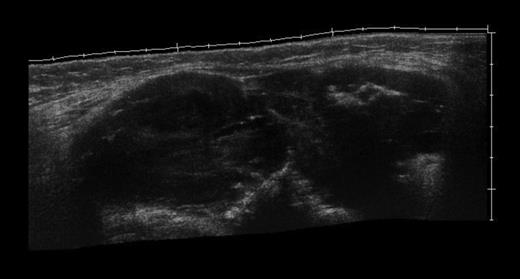
Ultrasound image showing heterogenous mass between the two heads of gastrocnemius muscle.
The MRI scan of the right knee (Figs 2 and 3) with gadolinium-enhancement showed a large mass lesion in the posterior aspect of the right knee extending into the popliteal fossa and into the upper third of the right leg having appearance of bursal pathology. Post gadolinium images showed evidence of circumferential rim enhancement but no internal enhancement indicating the presence of a fluid filled lesion. The mass (Figs 4 and 5) measured ∼8.39 × 6.14 × 12.72 cm and was seen between semimembranosus and biceps femoris muscles. There was no evidence of any infiltration of either the sciatic nerve or the popliteal vessels. A likely diagnosis of complicated synovial cyst with a differential diagnosis of haematoma was reported and a provisional diagnosis of Baker's cyst was established.

T1-weighted MRI image showing mass occupying whole of posterior aspect of knee extending to proximal portion of the leg.
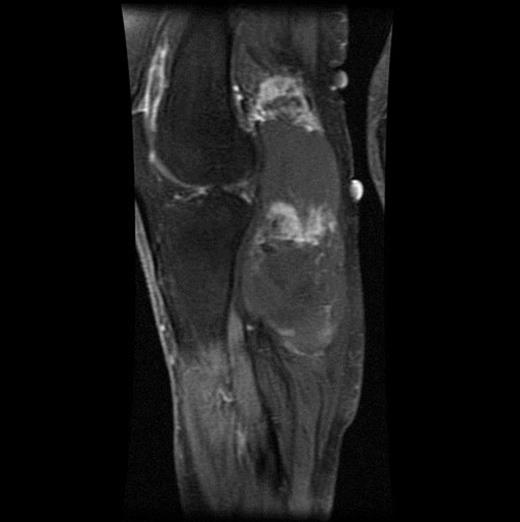
T2-weighted MRI image of the same mass lesion.
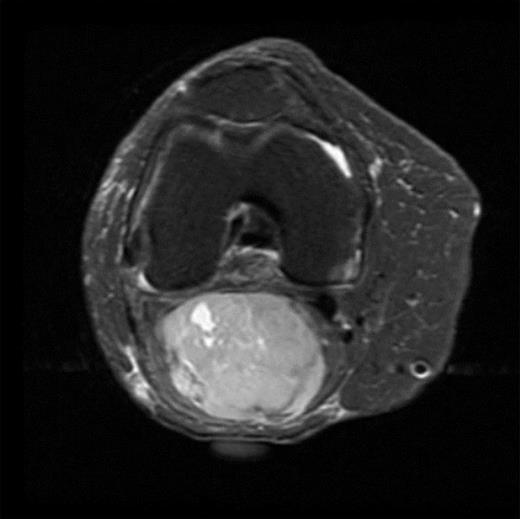
Axial MRI image of sarcoma.
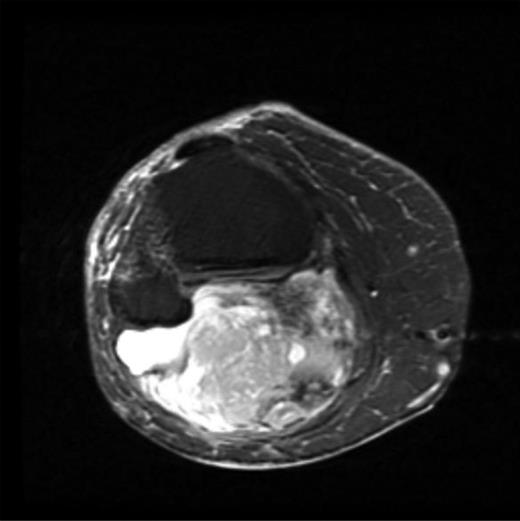
Post gadolinium-enhanced MRI image showing circumferential lesion.
She was admitted a month later in the medical ward with right leg swelling to rule out deep vein thrombosis. On admission, she had calf tenderness, right lower leg pitting oedema, mild erythema around the foot and ankle and faint peripheral pulses. Venogram ruled out deep vein thrombosis and X-ray of the knee revealed extensive ill-defined calcification within the soft tissue mass in the popliteal fossa extending posteriorly to the proximal tibia but no other bony abnormality was found.
Two months later she was admitted under vascular surgeons with critical ischaemia of the right leg. Doppler examination revealed swollen calf, reduced sensation in the foot and absent pulses in posterior tibial and dorsalis pedis arteries.
An urgent incisional biopsy of the popliteal mass was performed, which revealed soft tissue sarcoma (STS). A CT scan confirmed soft tissue mass consistent with STS in the popliteal fossa with metatstasis to the lungs and stomach.
Patient was offered above-knee amputation which she declined and subsequently developed gangrene of her foot. This patient had a rapid worsening of her symptoms over a few months but unfortunately her diagnosis was delayed till she developed neurovascular compromise and already had secondary lesions implying a very poor prognosis and she chose not to have any intervention.
DISCUSSION
STSs are uncommon tumors of mesenchymal origin and represent ∼1% of all adult cancers [3]. The extremities represent one of the most common primary sites for STS, but the popliteal fossa is a relatively rare anatomic site of primary tumor presentation that presents unique management challenges [4]. Treatment typically involves a multidisciplinary approach, but adequate surgical resection remains the mainstay of primary local therapy for this type of tumour, and previous studies have reported that tumor size and grade are important factors for survival [4, 5].
Patients may not have classical presenting symptoms of malignancy like constitutional symptoms, weight loss or loss of appetite. However, any finding of reduced vascularity needs to be vigorously investigated. Sudden increase in size of lump, change in consistency, increased pain and neurovascular compromise are all red flags that indicate a need for thorough assessment.
Different signal intensities of MRI can assist in differential diagnosis of lesions around the knee, STSs appear as heterogenous lesions on MRI, whereas Baker’s cyst typically has uniform hypointense signal on T2-weighted images and hyperintense on T1-weighted images as a result of their high water content [6]. Plain X-rays although not diagnostic should raise a suspicion of malignancy if there is irregular calcification. Ultrasound provides a quick and cheap screening tool to discover the contents of the swelling, and any abnormal echo signals should prompt further evaluation in the form of MRI scan. Histopathology remains the gold standard in diagnosing these lesions.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}