





Abstract
Duodenal rupture secondary to blunt trauma is a relatively uncommon event and is usually a result of a road traffic accident. As the duodenum is a retroperitoneal organ, delays in diagnosis can occur, as the patient may present with vague abdominal symptoms and other non-specific signs. Computed tomographic scanning is therefore a useful tool in the diagnosis of this condition. We present a 19-year-old girl who was hit in the abdomen with a football and subsequently had a duodenal rupture.
INTRODUCTION
Blunt trauma to the abdomen is an uncommon cause of duodenal rupture. We report the case of a 19-year-old female football spectator who suffered a duodenal rupture as a result of being hit in the abdomen by a football.
CASE REPORT
A 19-year-old girl presented to the Emergency Department at 1 am after having a football kicked from a distance of 5–10 m into her abdomen 7 h previously whilst watching a game. She complained of worsening diffuse abdominal pain and vomiting. Her observations were stable; however, on examination, her abdomen was diffusely tender and there was evidence of generalized peritonism. She had a white cell count of 18.8 × 109/l, but the rest of her blood tests, including amylase, was normal. Her chest radiograph did not show any evidence of free air under the diaphragm. A computed tomographic (CT) scan of her abdomen and pelvis was arranged, which showed abnormal areas of low attenuation and multiple pockets of air in the right flank, surrounding the right kidney and in the right sub-hepatic space, consistent with a perforation of either the ascending colon or the duodenum (Fig. 1). A laparotomy was performed and a 0.5 cm perforation was seen in the antero-lateral border of the duodenum at the junction of the first and second parts of the duodenum following kocherization. The perforation was oversewn and repaired with an omental patch. She recovered well from the operation and was discharged 4 days later.
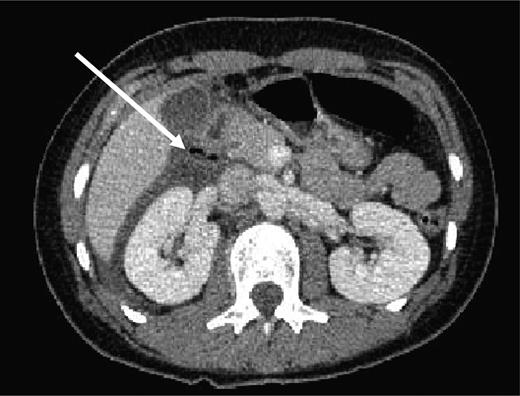
CT of abdomen showing free air in right para-renal space (white arrow).
DISCUSSION
The duodenum is a ‘C’-shaped organ primarily situated in the retroperitoneum and is anatomically divided into four sections (D1–D4). It is vulnerable to damage by shearing or compression forces, as D1 and D4 are relatively mobile in comparison with D2 and D3, which are fixed. Commonly injuries occur at the junction between D3 and D4 and at the junction between D1 and D2, as seen in this case [1, 2]. The retroperitoneal nature of the duodenum may also result in delays in the diagnosis of duodenal rupture as patients may not present with frank peritonism initially. It is therefore important to consider both mechanism of injury and also other clinical signs such as tachycardia and raised white cell count as delays in diagnosis and subsequent management have been shown to adversely affect morbidity and mortality [1–8]. However, in this case, due to the positioning of the perforation, duodenal contents entered the peritoneal cavity directly from the point of rupture, thus causing peritoneal irritation.
Duodenal injuries secondary to blunt trauma can range in severity from an intramural haematoma to a complete transection and devascularization of the duodenum, and are graded 1–5 by the American Association for Surgery of Trauma [2, 5, 6]. CT scanning is a useful adjunct to in the diagnosis of duodenal rupture, and can aid in the differentiation between full thickness rupture that requires surgical intervention and a haematoma which can be managed conservatively. The finding of fluid in the right anterior para-renal space on a CT scan may be seen in the presence of a duodenal haematoma, whereas if air is seen in this area duodenal rupture is likely to have occurred [1–4, 6, 9]. In this case, CT scanning was useful in delineating the possible area where a perforation may be found, especially as the patient presented with generalized abdominal pain. There are multiple ways to repair a duodenal rupture and these are obviously dependant on the severity of the injury. The literature suggests that kocherization (mobilization) of the duodenum should be performed to allow full examination of the duodenum to rule out multiple perforations [1, 2, 4, 7, 9].
Duodenal perforations are uncommon secondary to blunt trauma, comparative to penetrating trauma. A retrospective study analysing a trauma database of 103,864 patients showed that only 0.2% (208 patients) had a duodenal injury related to blunt trauma and of these only 30 patients had full thickness duodenal rupture. The most common mechanism of injury was involvement in a road traffic accident [1, 3]. Duodenal rupture as a result of a sporting injury is very rare and there are no reports of duodenal injury from the specific mechanism described in this report [8, 10].
Duodenal rupture secondary to blunt trauma is a rare but significant event. This case demonstrates that even if the mechanism of injury seems trivial, a high level of suspicion should be maintained in the presence of suggestive clinical findings. It also shows the benefit of CT scanning in the diagnosis and management of duodenal rupture.

{kind=link}
{kind=link}