





Abstract
Gallstone ileus is an uncommon complication of cholelithiasis, usually associated with an internal biliary fistula. Management of gallstone ileus is surgical with enterolithotomy the procedure of choice, followed by fistula closure either as a one or two stage procedure. In this case a 66 year old female presented with colicky abdominal pain, computed tomography (CT) clearly showing a gallstone ileus and cholecystoduodenal fistula. Despite this the patient refused surgery and went on to have spontaneous resolution of the obstruction and passage of gallstones.
INTRODUCTION
Gallstone ileus is an uncommon complication of cholelithiasis. It accounts for 1-4% of mechanical small bowel obstruction, and up to 25% of non-strangulated small bowel obstruction in patients >65 years age (1,2). Gallstone ileus is usually associated with an internal biliary fistula as >90% of obstructing stones are >2cm, therefore too large to pass through the common bile duct (3). There are some reports of gallstone ileus without fistula following endoscopic sphincterotomy (4).
CASE PRESENTATION
A 66 year old female presented with a three month history of intermittent epigastric pain which had increased in intensity over the previous two weeks, and was accompanied by bloating, nausea, and vomiting. She had a history of hypertension and type II diabetes, with no other significant medical or surgical history.
On examination the abdomen was mildly distended though soft, with active bowel sounds. Laboratory results were unremarkable. Plain abdominal radiograph showed pneumobilia. A subsequent CT abdomen (figure 1) showed a thick walled gallbladder with inflammatory changes and a fistula to the adjacent duodenum. Also demonstrated was a >2cm gallstone within the caecum, along with four smaller stones within the terminal ileum, and features of small bowel obstruction.
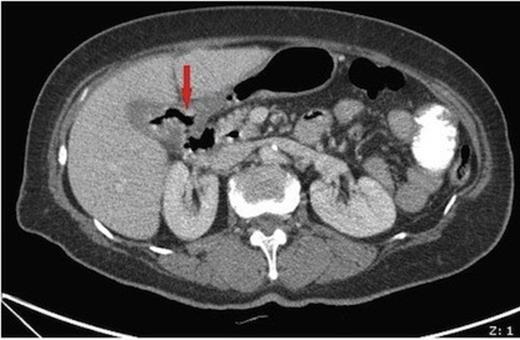
Axial CT image showing a thick walled gallbladder with inflammatory changes and a fistula to the adjacent duodenum
The patient refused surgery, and was managed conservatively. She was discharged home following spontaneous resolution of the ileus. She did not present for follow-up, and we can only assume all the gallstones were passed spontaneously and the patient has remained complication free.
DISCUSSION
Internal biliary fistulas are an uncommon complication of gallstones with a reported incidence of 0.4-3.2% in patients with biliary disease(5,6). Most internal biliary fistulas are spontaneous, and may be biliary-biliary, biliary-enteric, or broncho-biliary, the commonest being cholecystoenteric, including cholecystoduodenal (77%), cholecystocolonic (15%), and cholecystogastric (2%) (5). More than 90% of internal biliary fistulas are the result of calculi in gall bladder or bile ducts, with the remainder associated with penetrating peptic ulcer disease, malignancy, trauma, or Crohn's disease (5).
Biliary-enteric fistulas may form from a stone impacted in the bladder neck, with pressure necrosis causing an erosion through the gall bladder wall and fistula formation (5), or following an attack of cholecystitis where there has been pericholecystic inflammation resulting in adhesions formed between the biliary and enteric systems, and ischaemia leading to perforation of gallbladder contents into the adjacent viscus.
Diagnosis of gallstone ileus is often difficult as findings are nonspecific, with many patients proceeding to operation without a diagnosis. Rigler's triad of radiologic findings (pneumobilia, extra-biliary gall stone, & small bowel dilatation) may be useful, though only occurs in 50% of cases (2). Most present with features of uncomplicated gallstone disease, and cholecystitis often complicates cholecystocolonic and cholecystogastric fistulas in 60% and 40% respectively (7). In about 50% there is a history of jaundice, either in the past or at presentation, and loose bowel motions may be associated with a cholecystocolonic fistula (7) Severe haemorrhage complicating cholecystoduodenal fistula has also been reported (7).
Although there has been report in the literature of successful conservative management of gallstone ileus (8), gallstone ileus is managed surgically. The procedure of choice is enterolithotomy, with or without fistula closure. There has been some debate of whether a one stage or two stage procedure is the preferred option, with a one stage procedure including cholecystectomy and definitive closure of fistula at the time of enterolithotomy. The one stage procedure has the advantages of not subjecting the patient to repeated procedures and hospitalisation, though mortality is higher in the one stage procedure (16-25%) vs. two stage (11-15%) (1,9). The high mortality is likely due to advanced age and many patients having serious co-morbidities, with up to 86% having an American Society of Anesthesiology class III or IV (2), and the long complex nature of the one stage approach.
For these reasons, many authors now advocate a two stage procedure, performing the fistula closure when the patient has been optimised, except in selected low risk patients (1,2,9). Closure of the fistula remains very important, as failure to perform a definitive closure of the fistula is associated with higher long term morbidity (10-11%), than those with cholecystectomy and fistula closure (0%) (1,9). Potential long term complications include cholangitis, cholecystitis, recurrent ileus, and an increased incidence of gall bladder cancer (1). More recently, successful laparoscopic techniques for closure of biliary-enteric fistulas have been described, with endoscopic stapling the procedure of choice (7,10).
Findings of a gallstone ileus is an absolute indication for surgery, though due to advances in technique, laparoscopic approaches to enterolithotomy and cholecystofistulectomy may be used by those sufficiently skilled. We report here, however, a case of successful conservative management in a patient not willing to undergo surgery.

{kind=link}