





Abstract
Heterotopic pregnancy (HP), defined as the coexistence of intrauterine and extrauterine gestations, is a rare but potentially life-threatening condition. Its incidence is estimated at 1 in 30 000 spontaneous pregnancies, while assisted reproductive technology (ART) markedly increases prevalence, reaching up to 1% after in vitro fertilization (IVF). Diagnosis is challenging since nearly half of patients remain asymptomatic until rupture, and the presence of an intrauterine pregnancy may mask the ectopic component. We report a case of HP in a 25-year-old woman with severe untreated hypothyroidism post-thyroidectomy, who conceived spontaneously without ART. She presented with hemoperitoneum from a ruptured interstitial pregnancy and underwent emergency laparotomy with salpingectomy. Despite initial preservation of the intrauterine pregnancy, fetal demise occurred later. This rare association underscores the importance of maintaining a high index of suspicion for HP even in the absence of risk factors and raises questions about whether thyroid dysfunction may contribute to abnormal implantation.
Introduction
Heterotopic pregnancy is defined as the simultaneous occurrence of intrauterine and ectopic gestations [1, 2]. It carries a high risk of maternal morbidity and potential loss of the intrauterine pregnancy [3]. Although spontaneous incidence is extremely low, ART and ovulation induction significantly increase the risk [4, 5]. Diagnosis is often delayed because symptoms are nonspecific, and visualization of an intrauterine pregnancy may obscure the ectopic component [6, 7]. Transvaginal ultrasonography usually detects cases between 5–8 weeks, with color Doppler improving accuracy [2, 8, 9]. However, misinterpretation remains common, particularly in resource-limited settings.
We present a rare case of HP in a woman with severe untreated hypothyroidism after total thyroidectomy, who conceived spontaneously without conventional risk factors.
Case presentation
A 25-year-old Caucasian woman, gravida 2 para 0 (G2P0A1), at 10 weeks’ gestation presented with a 3-day history of lower abdominal pain and scant brown vaginal spotting. She had a prior first-trimester miscarriage at 12 weeks and conceived spontaneously without ART. An ultrasound performed two weeks earlier confirmed a viable intrauterine pregnancy.
The patient had undergone total thyroidectomy three years earlier for a thyroid cyst and had not received adequate thyroid hormone replacement. At conception, TSH was markedly elevated (109 μIU/mL), and levothyroxine 150 μg daily was initiated, though follow-up was inadequate. She had no history of pelvic inflammatory disease, pelvic surgery, or ovulation induction.
On admission, she appeared pale with mild abdominal tenderness. Vital signs: BP 90/60 mmHg, pulse 91 bpm, temperature 37°C, SpO₂ 95%. Transvaginal ultrasound demonstrated a 10-week intrauterine pregnancy with positive cardiac activity (Fig. 1); adnexa were not assessed. Initial labs showed anemia (Hb 9.1 g/dL) and leukocytosis (WBC 13000/μL).

Transvaginal ultrasound showing a 10-week intrauterine pregnancy with positive cardiac activity.
Within 24 hours, she developed severe abdominal pain, pallor, tachycardia (130 bpm), and hypotension (60/40 mmHg). Repeat ultrasound revealed massive intraperitoneal free fluid consistent with hemoperitoneum, while intrauterine fetal cardiac activity persisted. Hemoglobin dropped to 6.9 g/dL. Due to hemodynamic instability and the large hemoperitoneum, detailed adnexal assessment was not feasible.
Emergency laparotomy evacuated approximately 2.5 L of hemoperitoneum. A ruptured interstitial ectopic pregnancy of the left tube was identified (Fig. 2), and left salpingectomy was performed (Fig. 3). Blood transfusion and peritoneal lavage were administered.

Intraoperative findings of ruptured left interstitial ectopic pregnancy with hemoperitoneum.
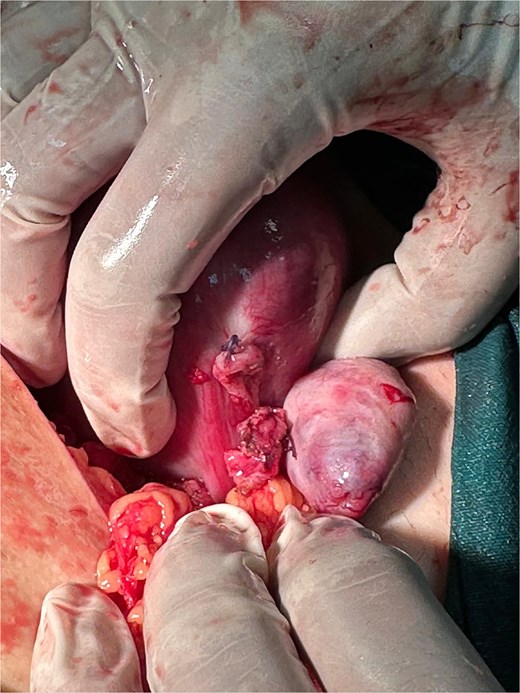
Intraoperative view after suturing of the ruptured left interstitial site following salpingectomy and hemostasis.
Postoperatively, the patient stabilized (BP 110/70 mmHg, pulse 86 bpm). Histopathology confirmed tubal ectopic pregnancy, consistent with the intraoperative diagnosis of a ruptured interstitial pregnancy. Gross examination revealed a ruptured tubal segment with adherent hemorrhagic clots. Microscopic examination demonstrated chorionic villi and associated trophoblastic tissue within the fallopian tube wall, accompanied by extensive hemorrhage (Fig. 4). No evidence of malignancy was identified. Despite postoperative progesterone supplementation, intrauterine fetal demise occurred two weeks later, necessitating dilation and curettage.
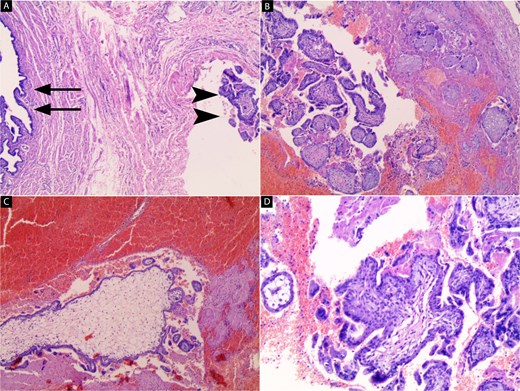
Histopathological examination of the resected left fallopian tube (H&E stain). (A) Low-power view showing the fallopian tube lumen (arrows) with chorionic villi embedded within the tubal wall (arrowheads) (40x). (B) Chorionic villi within the tubal wall associated with surrounding hemorrhage (40x). (C) Chorionic villus with extensive surrounding hemorrhage (40x). (D) Higher magnification revealing chorionic villi lined by trophoblastic cells confirming ectopic pregnancy (100x).
Discussion
Heterotopic pregnancy (HP) is a rare obstetric emergency, first described in 1708 [1]. It results from simultaneous intrauterine and ectopic implantation, most commonly in the fallopian tube [10]. The spontaneous incidence is estimated at ~1 in 30 000 natural conceptions, but the rate increases significantly with assisted reproductive technology (ART), reaching up to 1% after in vitro fertilization (IVF) [4, 7]. Known risk factors include pelvic inflammatory disease, previous ectopic pregnancy, endometriosis, intrauterine device use, pelvic surgery, and ART-related embryo transfer [6, 11, 12]. Nevertheless, around 20% of cases occur without identifiable risk factors [1], as in our patient, highlighting the unpredictability of this condition.
The clinical presentation is frequently nonspecific, with abdominal pain, vaginal bleeding, and amenorrhea being common manifestations that may mimic miscarriage or ovarian cyst rupture [1, 10]. Importantly, about half of patients remain asymptomatic until rupture occurs [6]. In our case, the initial presence of a viable intrauterine pregnancy contributed to diagnostic delay, underscoring the importance of systematically assessing the adnexa even when intrauterine gestation is confirmed. Transvaginal ultrasonography between 5–8 weeks remains the cornerstone of diagnosis [2, 8]. The addition of color Doppler improves sensitivity, yet false negatives are still common, particularly in resource-limited settings [7, 9, 13].
Management is individualized according to hemodynamic stability, site of implantation, and desire for fertility preservation. Laparoscopy is the preferred approach in stable patients, whereas laparotomy is required in unstable cases [1, 2, 4]. In our patient, massive hemoperitoneum necessitated emergency laparotomy and salpingectomy. Despite initial preservation of the intrauterine pregnancy, fetal demise occurred—a complication reported in up to 25% of HP cases [14]. Live birth rates of 60%–70% have been described following timely intervention [2].
Most published reports of HP are linked to ART or predisposing pelvic factors [5, 7, 12]. Spontaneous heterotopic pregnancy without such risks is exceedingly rare. Furthermore, published cases emphasize the diagnostic challenge when intrauterine pregnancy is visualized, often leading to late recognition and rupture [3, 6, 15]. Our case is consistent with these findings, as diagnosis was established only intraoperatively following hemodynamic collapse. The diagnosis was confirmed histologically by identification of chorionic villi and trophoblastic tissue within the resected fallopian tube. Hypothyroidism is known to impair fertility through mechanisms such as anovulation, luteal phase defects, hyperprolactinemia, and impaired endometrial receptivity [16]. Thyroid hormones also play roles in angiogenesis and trophoblastic invasion during early implantation. Severe untreated hypothyroidism, as in our patient, may disrupt these processes and contribute to abnormal implantation. While hypothyroidism has been strongly associated with miscarriage, preterm delivery, and fetal demise [16], to our knowledge, no previous reports have linked it directly to heterotopic pregnancy.
The uniqueness of this case lies in the coexistence of heterotopic pregnancy with severe untreated hypothyroidism in a young woman without conventional risk factors or ART exposure. This rare association raises the possibility that endocrine dysfunction may represent a previously unrecognized contributor to abnormal implantation. It underscores the importance of maintaining high clinical suspicion for HP even in the absence of risk factors, and highlights the need for further studies to explore the relationship between thyroid dysfunction and implantation abnormalities.
Conclusion
Heterotopic pregnancy is a rare but potentially fatal condition that requires high clinical suspicion, even when an intrauterine gestation is present. Early transvaginal ultrasonography with careful adnexal evaluation is essential for timely diagnosis. Management depends on maternal stability and fertility goals, with surgery remaining the mainstay in emergencies.
This case is unique in demonstrating HP in a patient with severe untreated hypothyroidism, suggesting a possible novel risk factor. Further research is needed to clarify the role of thyroid dysfunction in abnormal implantation and heterotopic pregnancy pathogenesis.
Conflicts of interest
No conflict of interest.
Funding
There was no funding for this publication.
Ethical approval
No ethical approval was required for this publication.
Consent
Informed and written consent from the patient was taken prior to publication.

{kind=link}
{kind=link}
{kind=link}
{kind=link}