





Abstract
Spontaneous femoral artery pseudoaneurysm is a rare disease and reported cases are very few. Most of them are related to underlying pathology either atherosclerotic disease or connective tissue disease. We present a 29-year-old healthy man with two months history of a painful pulsating mass at the level of the lower right thigh without any previous history of trauma, surgery or puncture of the femoral artery. An angiogram revealed a right superficial femoral artery pseudo-aneurysm. It was treated surgically by resection of the aneurysm, reconstruction with inter-positional saphenous vein graft. We reported this case because of its rare incidence in the young patient with no underlying pathology.
INTRODUCTION
Spontaneous pseudoaneurysm of the femoral artery is extremely a rare entity.(1) It can be secondary to the rupture of a true aneurysm, but in most events the cause is unclear.(2) Most patients with non-atherosclerotic pseudoaneurysms of SFA are asymptomatic initially and later present with a pulsatile, expanding mass along the anatomical course of SFA in the thigh and have a history of some trauma or surgical procedure.(3) Due to their complications, large pseudoaneurysms require some kind of intervention. If not treated, they are at risk for rupture, infection, distal embolization or arteriovenous fistula formation. (1) We report a young patient with spontaneous femoral artery pseudoaneurysm without any history of trauma or vascular intervention successfully treated surgically.
CASE REPORT
A 29-year-old healthy man presented with right thigh swelling since 2 months which is painful throbbing in nature and aggravated by walking. This swelling has increased in size rapidly over last one month. No history of rest pain but mild claudication on running. There was no history of local trauma and he had never suffered peripheral vascular disease.
On presentation, he was hemodynamically stable and there was a tender swelling at the medial aspect of right mid thigh which was pulsatile. The pedal pulses were intact at the same side. Neurological exam was intact. No oral, genital ulcers or other physical findings to suggest connective tissue disease. There was no family history of cardiovascular diseases.
CT angiogram was done which showed a pseudoaneurysm of the lower third of femoral artery.
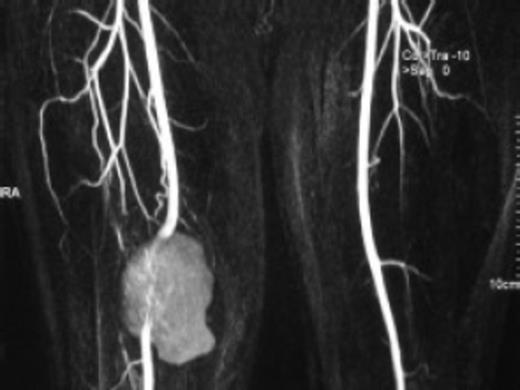
CT angiogram showed a pseudoaneurysm of the lower third of femoral artery
A surgical excision of the pseudo-aneurysm was done under general anesthesia. After evacuation of hematoma, there was a large defect in the wall of the artery. Therefore, a greater saphenous vein interposition graft was used to maintain the vascular continuity. He had an uneventful recovery. The histopathology confirmed our diagnosis of pseudoaneurysm with the absence of the arterial wall.
DISCUSSION
Formation of a femoral artery pseudoaneurysm is not infrequent after femoral arterial access, and it occurs in up to 0.7% of the diagnostic procedures and in up to 8% of the interventional procedures. (4)
Recently, there has been a significant decrease in both major and minor vascular complications after diagnostic and therapeutic procedures with an incidence of pseudoaneurysm less than 0.3 %. (5)
Spontaneous pseudoaneurysm of the superficial femoral artery in the young age group is a rare occurrence. Femoral artery pseudoaneurysms have been described following various vascular interventions. Some of the false aneurysm may close spontaneously but rupture is a major concern followed by thrombosis, distal embolization and compression of adjacent structures. Christos et al has described a thigh compartment syndrome due to a false aneurysm. (3)
Atherosclerosis has been proposed by several authors as an etiologic factor in spontaneous perforation of the femoral arteries or its branches. (6-8) In these case reports, the patients were elderly with atherosclerotic changes in their peripheral arteries and weakening of the arterial walls could have led to spontaneous rupture. Patients who have inherited connective tissue disorders such as Ehlers-Danlos have also been reported to present with spontaneous rupture of their arteries because of the fragility of their arterial walls. (9). Our patient, however, was young and there was no evidence of atherosclerotic changes in his arteries on the angiogram or during surgery. Furthermore, he did not have any clinical features to suggest an inherited connective tissue disorder. There was also no history for any trauma and for which we labeled him to have a spontaneous femoral artery pseudoaneurysm.
Therapeutic options for femoral pseudoaneurysm include open surgical repair, ultrasound-guided compression, ultrasound-guided thrombin injection, coil embolization, and endovascular repair using stent-grafts. (10) Particularly in young patients, an appropriate approach is surgical exploration with hematoma evacuation and arterial repair by means of arterial suture, patch angioplasty, or graft interposition. (2)
Femoral artery pseudoaneurysm has been a common complication after the wide use of femoral artery access for diagnostic and therapeutic procedures. However, spontaneous rupture of the artery without trauma remains a rare entity. As there are many evolving types of management, the surgical intervention may has superiority when there is a suspicious of underlying vascular pathology.

{kind=link}