





Abstract
A 62-year-old man presented with a 6-week history of shortness of breath, weight loss and painful swelling of the great toe. Examination elicited an ulcerated swelling of the right great toe, thought to be an ingrowing toenail. Chest ‘crackles’ and an enlarged supraclavicular lymph node were detected. Biopsies of the toe swelling and bronchi both showed squamous cell carcinoma, confirmed radiologically as stage IV lung cancer. The patient was referred for palliative amputation of the toe. Cancer metastases to the digits may arise in bone, before enlarging to invade skin, or arise in skin first. 20-60% of cutaneous metastases present before or at the same time as the primary lung tumour. Cutaneous metastases and those in the digits indicate very poor prognosis. Their prompt diagnosis and management can dramatically improve a patient’s quality of life and should be strived for.
INTRODUCTION
Cutaneous metastasis of lung tumours are rare, occurring in 0-4% of cases (1). They indicate a very poor prognosis; mean survival has been reported as 5-6 months (2). Metastases to the digits may initially arise in bone, before enlarging locally to invade skin, or arise in skin first (3).
We describe the case of a non-small cell lung cancer presenting as metastasis in the great toe, demonstrating how advanced the disease may be at the time of presentation and how metastases may be mis-diagnosed. The clinical and pathological features of such metastases are discussed.
CASE REPORT
A 62-year-old male was admitted for investigations following a 6-week history of increasing shortness of breath, weight loss, and swellings of the right great toe and right elbow. His toe had felt hot for 6 weeks, and in the latter 2 weeks had discharged pus, become itchy and developed a burning sensation before becoming swollen. He had developed a productive cough, a reduced exercise tolerance and had recently given up smoking.
The patient’s medical history included chronic obstructive pulmonary disease, idiopathic pulmonary fibrosis and cerebrovascular disease. He was on appropriate medication including aspirin, his alcohol intake was minimal and he was a retired plasterer.
Examination showed a swollen, foul smelling raw area at the distal phalanx of right great toe with overlying slough. There was erythema and pain initially thought to be consistent with infection from an ingrowing toenail (Fig. 1). A firm, 3cm wide, rubber-like swelling was noted at the lateral aspect of the right elbow that was not tethered to skin, but was fixed to underlying structures. It was neither hot, red nor tender. Fine crackles were heard at the right lung base and there was an enlarged right supraclavicular lymph node and associated digital clubbing.

Clinical appearance of the right great toe at presentation.
A chest radiograph demonstrated consolidation in the right lower zone. X-ray of the right great toe (Fig. 2) showed destruction of the distal phalanx with adjacent soft tissue swelling, and of the right elbow showed soft tissue swelling over the lateral aspect with possible cortical destruction of the lateral epicondyle (Fig. 3).

Radiograph of right great toe demonstrating osteolysis of distal phalanx with adjacent soft tissue swelling but no periosteal reaction.

Radiograph of right elbow demonstrating a soft tissue swelling over the lateral epicondyle.
A CT scan showed an 8.8cm soft tissue mass occluding the right lower lobe bronchus (Fig. 4), bilateral nodules suspicious of pulmonary metastases, and lymphadenopathy in the right hilar, paratracheal and anterior mediastinal regions. In addition there were foci of reduced attenuation in the liver and thoracic skeletal metastasis with imminent cord compression at T4.
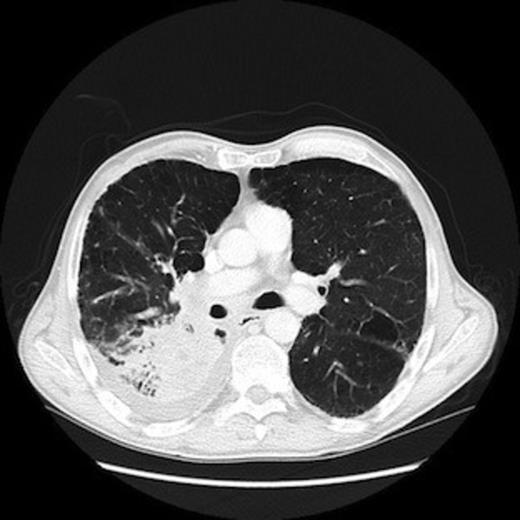
CT scan of chest demonstrating primary lung tumour in the right lower lobe.
Bronchoscopy demonstrated infiltrative irregular mucosa, highly suspicious of malignancy. Biopsy of this provided a histological diagnosis of squamous cell carcinoma. Punch biopsies of the ulcerated great toe swelling also showed squamous cell carcinoma. The presumed metastasis at the right elbow was not confirmed histologically as it was asymptomatic and the focus of treatment was elsewhere.
A staging of T4N3M1b (stage IV) non-small cell lung cancer was made following multidisciplinary discussion. The patient was referred to plastic surgeons for palliative amputation of the toe, which was undertaken 4 weeks following histological diagnosis. The patient reported an improvement in pain at the amputation site at first follow-up 1 week post-operatively. Due to a performance status of WHO grade 3 the patient was not a candidate for palliative chemotherapy, but five fractions of palliative radiotherapy were administered urgently to the T4 spinal metastasis, which allowed the patient to remain ambulant until his death 2 months following histological diagnosis. This survival time was shorter than the previously reported 5-6 months from detection of cutaneous metastases; some patients in the quoted studies had received chemotherapy(2).
DISCUSSION
Lung cancer is known to metastasize to all organ systems of the body (4), though skin is only the 12th most common site in non-small cell tumours (1). A review of 579 cases of lung cancer elicited cutaneous metastases in 16 (2.8%) of which all had accompanying metastases in other organs (5). In the latter study, a median survival of 4 months was observed following development of cutaneous metastases. As demonstrated well by this case, 20-60% of cutaneous metastases present before or at the same time as the primary lung tumour (2).
Metastasis to the digits is thought to mainly arise in the bone first, before enlarging locally to invade the skin but it can occur in skin first (3). The presentation is variable, but swelling, erythema, pain and fluctuance may be considered typical. Hence cutaneous metastases from many primary tumours are often confused with infection, inflammation, cysts, osteomyelitis and gout among other conditions (6), thereby delaying diagnosis. It is not clear whether the metastasis in this patient’s toe arose in the skin, bone, or other tissue. The histology report from the amputation stated that the tumour ‘invades bone’, implying that it’s tissue of origin was outside the bone. Certainly the clinical appearance was in keeping with a cutaneous metastasis.
A series of 133 digital metastases from various types of primary tumour showed only 8% occurred as solitary metastases in the great toe, compared to 86% in the fingers (3). The rarity of digital metastasis is thought to be due to the relative absence of red marrow in the digital bones.
The mechanism by which lung cancer metastasises to distal peripheries is thought to be via extension through the valves of the vertebral venous system, to lumbar spinal and iliofemoral veins in which incompetent valves allow distal passage of emboli, aided by gravity (3). Interestingly, the tumour in this case seemed to almost exclusively involve the right side of the patient’s body, which given the above proposed mechanism, may not be entirely due to chance. It has also been suggested that chemotactic factors released following trauma may contribute to migration of tumour emboli and adherence to injured tissue (7), and the great toe is a frequently injured site.
This case highlights how advanced lung cancer may be at the time of presentation, with multiple widespread distant metastases presenting in a narrow time period. Cutaneous metastases and those in the digits indicate a very poor prognosis, with palliative treatment frequently being the only option. A diagnosis of metastatic disease should be considered in patients with risk factors for, or known cancer, particularly when microbiological anaylsis and antibiotic treatment for presumed infection has failed to improve symptoms. Prompt diagnosis and management of these metastases can dramatically improve a patient’s quality of life and should be strived for.

{kind=link}
{kind=link}
{kind=link}
{kind=link}