





Abstract
Proximal jejunal injuries after blunt abdominal trauma are rare and challenging to diagnose early, with delayed recognition increasing morbidity. Management depends on hemodynamic status, injury severity, and contamination, with resection and primary anastomosis recommended when more than 50% of bowel circumference is compromised. A 38-year-old female sustained blunt abdominal trauma in a traffic accident and presented hemodynamically stable with peritoneal signs, leucocytosis, elevated inflammatory markers, and free intraperitoneal air. Laparotomy revealed a proximal jejunal perforation involving over 50% of the circumference, 10 cm distal to the ligament of Treitz. Segmental resection with primary anastomosis and abdominal lavage with two drains was performed. Recovery was uneventful, with bowel function returning on postoperative day (POD) 2 and discharge on POD 10. Follow-up confirmed full recovery. Early recognition and timely surgery are crucial, and primary anastomosis is safe in stable patients with significant circumferential injury.
Introduction
Small bowel injuries account for a minority of blunt abdominal trauma cases but carry significant morbidity when diagnosis is delayed. The proximal jejunum, particularly near the ligament of Treitz, is vulnerable to deceleration forces and compression against the spine. Early identification remains challenging due to nonspecific symptoms and subtle imaging findings [1–3].
According to the World Society of Emergency Surgery (WSES), management of small bowel trauma depends on hemodynamic stability, injury severity, and degree of contamination [1]. Primary repair is appropriate for small perforations involving <50% of the circumference, whereas resection with anastomosis is recommended for larger defects or devascularized segments [1, 4]. The small bowel’s excellent healing capacity supports primary anastomosis in most trauma settings, with reported leak rates around 3% [1, 3].
We present a case of isolated proximal jejunal perforation near the ligament of Treitz following blunt trauma, managed successfully with resection and primary anastomosis.
Case presentation
A 38-year-old female was transferred from a provincial hospital to the national hospital after sustaining blunt abdominal trauma in a traffic accident. On arrival, she was hemodynamically stable but complained of severe abdominal pain. Physical examination revealed generalized abdominal tenderness with peritoneal signs.
Laboratory investigations showed leucocytosis with elevated neutrophils and markedly increased C-reactive protein. Upright abdominal X-ray demonstrated free intraperitoneal air, raising suspicion for hollow viscus perforation (Fig. 1).

Upright abdominal X-ray demonstrating free intraperitoneal air.
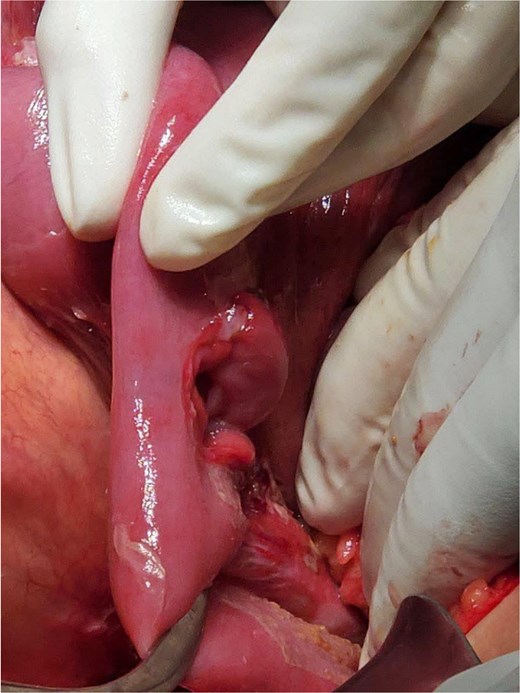
Given the clinical and radiologic findings, the patient was taken for emergency exploratory laparotomy. Intraoperatively, a perforation involving more than 50% of the circumference of the proximal jejunum was identified ~10 cm distal to the ligament of Treitz (Fig. 2). The surrounding bowel was edematous, but viable (Fig. 3).

Proximal jejunal perforation located near the ligament of Treitz.
Edematous but viable proximal jejunal loops.
Segmental resection of the affected jejunal segment was performed, followed by primary end-to-end anastomosis. The peritoneal cavity was thoroughly irrigated, and two drains were placed—one in the Douglas pouch and one in the sub splenic space.
Postoperatively, the patient recovered uneventfully. Return of bowel transit occurred on postoperative day (POD) 2, and both drains were removed on POD 3 (Fig. 4). On POD 5, laboratory tests demonstrated normal WBC (6.3 × 109/l) with neutrophil predominance, normal hemoglobin and platelets, normal renal function, and only mild hyponatremia (Na 133 mmol/l). C-reactive protein remained positive but consistent with the expected postoperative inflammatory response. Overall, the POD 5 laboratory profile indicated good postoperative progress with no evidence of sepsis or anastomotic leak (Table 1). She received analgesics and a 10-day course of ceftriaxone and metronidazole. The surgical wound remained clean throughout hospitalization. She was discharged on POD 10 in good condition and demonstrated full recovery on follow-up.

Clean postoperative wound on POD 3 and drain removal.
POD 5 laboratory results.
| Parameter | Result | Unit | Reference range | Interpretation |
|---|---|---|---|---|
| WBC | 6.3 | ×109/l | 4–10 | Normal |
| Neutrophils | 82% (5.17) | % (×109/l) | 1.4–7 | Neutrophil-predominant pattern |
| Lymphocytes | 14% (0.88) | % (×109/l) | 1.2–3.8 | Mild lymphopenia |
| Monocytes | 3% (0.19) | % (×109/l) | 0.1–1 | Normal |
| Eosinophils | 1% (0.06) | % (×109/l) | 0.02–0.5 | Normal |
| Basophils | 0% (0.00) | % (×109/l) | 0–0.1 | Normal |
| Hemoglobin | 13.6 | g/dl | 12–15 | Normal |
| Hematocrit | 41.1 | % | 36–45 | Normal |
| Platelets | 314 | ×109/l | 150–450 | Normal |
| Glucose (random) | 150 | mg/dl | 79–140 | Mildly elevated (stress response) |
| Sodium | 133 | mmol/l | 135–145 | Mild hyponatremia |
| Potassium | 4.1 | mmol/l | 3.5–5.1 | Normal |
| Chloride | 98 | mmol/l | 98–108 | Normal |
| Creatinine | 0.8 | mg/dl | 0.5–0.9 | Normal renal function |
| CRP | Positive | — | Negative | Expected postoperative inflammatory response |
Discussion
Proximal jejunal perforations after blunt trauma are rare but clinically significant. Mechanisms include rapid deceleration, compression against the vertebral column, and sudden increases in intraluminal pressure. Early diagnosis is essential, as delays beyond 8 h are associated with increased morbidity and mortality [1, 3, 4]. Primary repair is appropriate for small, single perforations involving <50% of the circumference with minimal contamination [1, 4]. Resection with anastomosis is indicated when >50% of the circumference is injured, when multiple perforations are present, or when mesenteric devascularization causes ischemia [1].
In this case, the perforation exceeded 50% of the circumference, making resection the appropriate choice.
The patient was hemodynamically stable, without severe contamination or physiologic derangement. WSES guidelines recommend primary anastomosis in Class A patients—those who are stable with minimal contamination—along with 3–5 days of antibiotics [1, 4, 5].
Damage control surgery is reserved for unstable patients, those requiring vasopressors, or those with severe contamination. Hemodynamic instability, vasopressor requirement, hypothermia, acidosis, and coagulopathy favor delayed anastomosis or stoma creation [1, 4].
The patient’s rapid return of bowel function and absence of postoperative complications align with reported outcomes for early primary anastomosis in stable trauma patients. Leak rates remain low (~3%) when performed under appropriate physiologic conditions [1, 3].
Conclusion
Proximal jejunal perforation near the ligament of Treitz is an uncommon but serious consequence of blunt abdominal trauma. Early recognition, prompt surgical exploration, and adherence to guideline-based decision criteria are essential for optimal outcomes. In stable patients with significant circumferential injury, resection with primary anastomosis is safe and effective. This case highlights the importance of timely intervention and structured decision-making in small bowel trauma.
Acknowledgements
The author wishes to express sincere gratitude to the Director of the National Maternal and Child Health Centre (NMCHC), Phnom Penh, Cambodia, for institutional support and guidance. Special thanks are extended to the surgical team and anesthesia team for their dedicated clinical care and collaboration, which made this study possible.
Author contributions
Chansokha Soeur (Conceptualization [lead], Writing—review & editing [lead])
Conflicts of interest
The authors declare no conflicts of interest.
Funding
No funding was received for this study. All resources were provided by the National Maternal and Child Health Centre (NMCHC), Phnom Penh, Cambodia.
Data availability
All data supporting the findings of this case report are included in the manuscript. Additional anonymized information may be made available from the corresponding author upon reasonable request and with institutional approval.
Ethical approval
This study received ethical approval from the Institutional Review Board of the National Maternal and Child Health Centre (NMCHC), Phnom Penh, Cambodia. All procedures were conducted in accordance with institutional guidelines and the ethical principles of the Declaration of Helsinki.
Informed consent
Written informed consent for participation and publication of clinical details was obtained from the patient.

{kind=link}
{kind=link}
{kind=link}
{kind=link}