





Abstract
Multicystic peritoneal mesothelioma (MCPM) is a borderline variant of peritoneal mesothelioma with indolent behaviour but a significant recurrence rate without radical treatment. Due to its rarity, risk factors and optimal treatment are still to clarify. The present clinical case is a report of MCPM developed after laparoscopic cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (Lap CRS-HIPEC) for pseudomyxoma peritonei (PMP) of appendiceal origin. The patient was treated for PMP with Lap CRS-HIPEC. One year later a recurrence was suspected at the thorax-abdomen computed tomography scan. After multidisciplinary discussion, she underwent iterative Lap CRS-HIPEC. Pathological examinations revealed MCPM. After 3 years of follow-up the patient is disease-free for both tumours. This is a unique case of MCPM mimicking recurrent PMP. Lap CRS-HIPEC is an effective approach for both conditions.
Introduction
Peritoneal mesotheliomas are rare malignancies exhibiting a wide range of clinical manifestations and levels of aggressiveness. Among the histological subtypes, multicystic peritoneal mesothelioma (MCPM) is typically regarded as a borderline form due to the high recurrence rate [1]. The report presents a case of a middle-aged woman diagnosed with MCPM 1 year following cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) for pseudomyxoma peritonei (PMP).
Case presentation
A 56-years-old woman was referred to our outpatient clinic after an open splenectomy. The histopathological examination of the specimen revealed a low-grade PMP. Post-operative abdomen computed tomography (CT)-scan confirmed the presence of left sub-diaphragmatic peripancreatic mucin deposits and a minimal free fluid in the pelvis. The patient’s medical history included a quadrantectomy for oestrogen receptor-positive ductal breast cancer, followed by radiotherapy and a 5-year course of Tamoxifen. Additionally, she had undergone bilateral ovariectomy for a benign ovarian cyst and a lung wedge resection for a benign lump.
After a multidisciplinary discussion, CRS-HIPEC was proposed. Preoperative investigation was completed with Upper GI endoscopy, colonoscopy, and abdominal magnetic resonance imaging (MRI). Laparoscopic CRS (Lap CRS-HIPEC) was performed including total omentectomy, appendicectomy, excision of small nodules of the mesosigma and right subdiaphragmatic peritonectomy. HIPEC regimen was Mitomycin C and Cisplatin administered for 60 minutes at target temperature of 41°C. The peritoneal cancer index (PCI) was 4. Histopathological examination confirmed the presence of PMP (grade 2) associated with a low grade appendiceal mucinous neoplasm (LAMN) (Fig. 1). The postoperative course was uneventful, and the patient was discharged 6 days after the CRS-HIPEC. Regular follow-up was planned with clinical examination every 3 months and thorax-abdomen CT scan every 6 months.
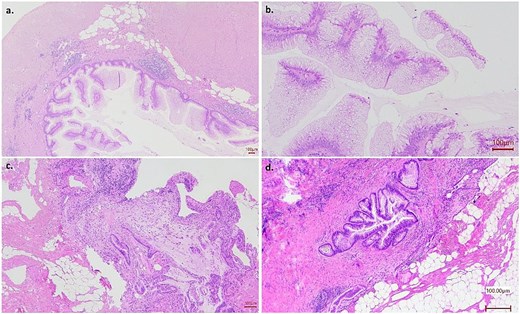
Low grade appendiceal mucinous tumour (LAMN) with pseudomyxoma peritonei grade 2. (a) Appendiceal fundus showing the presence of villous epithelial mucinous proliferation with low grade cytological atypia (b); pseudomyxoma peritonei of grade 2, showing peritoneal localization of low grade neoplastic mucinous epithelium with infiltrative pattern and moderate hypercellularity (c, d).
After almost 1 year the CT showed pelvic free fluid and pelvic plurilocular cysts suspected for disease recurrence. An abdominal MRI confirmed the findings (Fig. 2). After multidisciplinary discussion, an exploratory laparoscopy was proposed with cytoreduction and HIPEC if the disease recurrence was confirmed. The abdominal exploration confirmed the presence of multiloculated grape-like, fluid-containing cysts (Fig. 3) contiguous to the uterus and the cecum. No mucin was found. A complete resection was achieved with a fully laparoscopic approach. The intraoperative histological examination of the lesions was not conclusive for PMP. However, given the macroscopic appearance of the findings and the patient’s medical history, HIPEC with Cisplatin and Mitomycin C for 60 minutes was performed. No complications occurred and the patient was discharged after 5 days. The final histopathological examination revealed a multicystic lesion lined by flat-cuboidal epithelium without cytological atypia. Immunohistochemical analysis supported the mesothelial nature of the epithelial component which stained positive for calretinin and resulted negative for Podoplanin, CD31 and CDX2. Overall, the histopathological findings supported the diagnosis of MCPM (i.e. Multilocular peritoneal inclusion cyst, sec WHO 5th ed [2]) (Fig. 4).
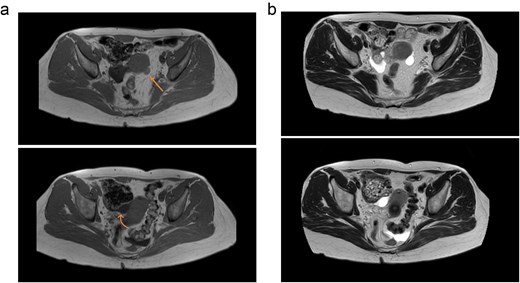
(a) Cystic lesions in T1-weightened MR images. Straight arrow indicates the cyst with haemorrhagic content, slightly hyperintense, whereas curved arrow the simple one. (b) Cystic lesions in T2-weightened MR images. In this sequence, the lesions are hyperintense.
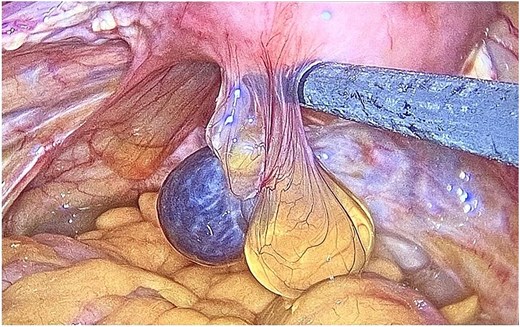
Intraoperative findings: Multiple cysts in pelvis with free fluid.
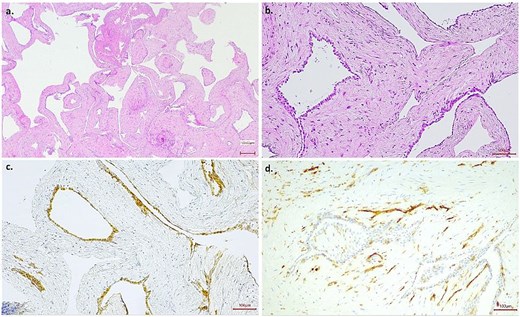
Multicystic peritoneal mesothelioma (i.e. multilocular peritoneal inclusion cyst, sec WHO 5th ed). (a) A multicystic proliferation with fibrous stroma; no infiltrative pattern nor stromal atypia was detected; (b) cysts were lined by flat-cuboidal epithelium without atypia which stained positive for calretinin (c) and negative for CD31 (lymphatic vessels as positive internal control) (d).
Discussion
MCPM has traditionally been considered a benign mesothelioma, and different theories have been proposed regarding its aetiology, with some authors suggesting an association with chronic peritoneal inflammation, such as that seen in conditions like endometriosis, previous abdominal surgeries, pelvic inflammatory disease [3], and familial Mediterranean fever [4]. Despite its slow growing nature, MCPM is associated with recurrence up to 50% after debulking surgery [5], and instances of malignant transformation have been described [6].
Mostly asymptomatic, patients with MCPM could complain vague abdominal pain or distensions, due to the progressive growth of the lesions. Urinary outflow obstruction or palpable mass have been reported [3]. MCPM appears as multiple grape-like cysts, from a few millimetres to over 20 cm, filled with clear serous fluid [7]. Comprehensive histopathologic evaluation by an expert pathologist is required to confirm the diagnosis and exclude differential diagnoses such as malignant mesothelioma, benign cystic lesions, lymphangioma, and endometriosis [8]. MCPM immunochemistry is usually positive for markers as Calretinin, WT-1, CK7, and D2–40 and variably for oestrogen and progesterone receptors [9]. Both Ki-67 and mitotic activity are low in MCPM when compared with the malignant counterpart and it could be explained by its pattern of growth [1]. Imaging could be helpful for differential diagnosis and both CT and MRI could provide information about the cysts, the extension, and the relationship with the surrounding organs, especially if they embed them. Lesions appear as multiple, most often located into the pelvis [10]. On MRI they appear as hypointense on T1 weighted images and mild to hyperintense in T2, although it may be the opposite in the case of cysts with a bloody content [3, 10].
Similar behaviour between MCMP and PMP—indolent development and a non-infiltrative pattern—suggests that the optimal treatment would be CRS-HIPEC [6]. Several studies had demonstrated excellent survival outcomes primarily using Cisplatin and Doxorubicin [7]. Firstly, Yan et al showed the impact of adding HIPEC to a complete CRS on disease control in a twelve patients’ multicentre study [5]. The study by Kepenekien et al [11] also showed that HIPEC was linked to a reduced incidence of recurrence and Nizri et al reported an 80% rate of disease-free survival at 10 years [12]. Reported recurrence rate ranges from 4% to 40%. The high recurrence rate and the potential for malignant transformation justify the aggressive treatment, despite ongoing debates regarding the neoplastic nature of the disease [8].
Lap CRS-HIPEC is a less invasive option to obtain a complete excision of peritoneal metastasis in selected cases [13]. The presented clinical vignette exemplifies an effective application of Lap CRS-HIPEC, both in PMP and MCPM, resulting in favourable postoperative outcome. The international PSOGI registry of Lap CRS-HIPEC reported nineteen cases of MCPM treated with this approach [14]. In a French study, 15 cases (25%) of Lap CRS-HIPEC for MCPM are reported. In this subgroup, median PCI was four and no recurrence was registered. No difference was shown regarding severe complications rate between open approach and Lap CRS-HIPEC, which was 27% and 7%, respectively [11].
Conclusion
The reported clinical case is a unique scenario of MCPM presented after a diagnosis of PMP. The unusual history of this patient remarks again the similarity between the two diseases in radiological and intraoperative features. Previous surgeries and intraperitoneal chemotherapy may have triggered the development of MCPM.
Conflicts of interest
None declared.
Funding
This research received ‘Ricerca Corrente’ funding from the Italian Ministry of Health to cover publication costs.
References

{kind=link}
{kind=link}
{kind=link}
{kind=link}