





Abstract
Pressurized intraperitoneal aerosol chemotherapy (PIPAC) is increasingly used for unresectable peritoneal metastases, although repeated laparoscopic access in patients with diffuse carcinomatosis may be technically challenging. We report our institutional experience with repeated PIPAC procedures, focusing on technical feasibility and reproducibility. Between December 2024 and December 2025, 24 PIPAC procedures were performed in 10 patients with ovarian and gastrointestinal malignancies. Despite hostile abdomens, intra-abdominal adhesions, and extensive peritoneal disease, all procedures were successfully completed laparoscopically without conversion to open surgery or major postoperative complications. Trocar positioning, selective cold-scissor adhesiolysis, reuse of previous access sites, and individualized CapnoPen® orientation contributed to maintaining procedural feasibility throughout repeated treatment cycles. Treatment interruption was mainly related to disease progression and deterioration of general clinical conditions rather than technical failure. Our experience suggests that repeated PIPAC is technically feasible and reproducible even in patients with advanced peritoneal carcinomatosis when careful surgical planning and tailored laparoscopic strategies are adopted.
Introduction
Peritoneal metastases represent an advanced stage of disease associated with poor prognosis and limited therapeutic options. Although cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy (CRS–HIPEC) may provide survival benefit in selected patients, many individuals are not candidates for such aggressive treatment because of extensive disease burden, previous treatments, or poor performance status [1, 2].
Pressurized intraperitoneal aerosol chemotherapy (PIPAC) was developed as a minimally invasive intraperitoneal drug delivery technique based on aerosolization of chemotherapeutic agents under pressure during laparoscopy [1]. Beyond potential oncologic benefits, one of the main theoretical advantages of PIPAC is the possibility of repeating procedures over time, allowing sequential reassessment of peritoneal disease and symptom control [3, 4].
However, repeated laparoscopic access in patients with diffuse carcinomatosis, previous systemic therapies, ascites, and intra-abdominal adhesions may represent a significant technical challenge. Real-world reports focusing specifically on the technical reproducibility of repeated PIPAC procedures remain limited [5–7].
The present study aimed to describe our institutional experience with repeated PIPAC procedures, focusing on technical feasibility, management of hostile abdomens, procedural reproducibility, and perioperative outcomes in patients with advanced peritoneal metastases.
Materials and methods
Study design
This retrospective observational study included patients undergoing PIPAC at our institution between December 2024 and December 2025 following multidisciplinary tumor board evaluation.
Patient selection
Patients with unresectable peritoneal metastases not eligible for CRS–HIPEC were considered for PIPAC within a multidisciplinary framework including surgeons, oncologists, radiologists, anesthesiologists, and pharmacists. Eligibility was based on performance status, disease burden, previous treatments, and feasibility of repeated laparoscopic procedures.
Surgical technique
All procedures were performed under general anesthesia using a laparoscopic approach. Abdominal entry was preferentially performed using an open technique in order to minimize the risk of bowel injury in patients with diffuse carcinomatosis, previous treatments, and hostile abdomens.
Trocar positioning was individualized according to previous surgical scars, adhesions, and distribution of peritoneal disease. In most cases, trocar configuration resembled standard laparoscopic cholecystectomy positioning. Particular attention was paid to maintaining reproducibility of abdominal access during repeated procedures, preferentially reusing previous trocar sites whenever feasible.
Initial exploratory laparoscopy was performed to assess feasibility of abdominal access and evaluate the Peritoneal Cancer Index (PCI). Dense adhesions and hostile abdominal conditions were frequently encountered during repeated procedures. Adhesiolysis was selectively performed using cold scissors in order to minimize thermal injury risk and was deliberately limited to what was necessary to safely obtain adequate working space and aerosol distribution.
Pneumoperitoneum was established using balloon trocars to reduce aerosol leakage. A dedicated scope-holder arm was used to stabilize the laparoscopic optic after definitive positioning of the CapnoPen® nebulizer.
The CapnoPen® device was directed toward areas with the highest macroscopic tumor burden or toward the distribution of the primary tumor. Chemotherapy aerosolization was delivered using a dedicated Medrad high-pressure injector adapted for PIPAC administration.
Oxaliplatin combined with doxorubicin was aerosolized under controlled pressure (12 mmHg) for 30 min at 37°C according to institutional protocol and ISSPP recommendations [3, 8, 9].
Follow-up and outcomes
The primary endpoint was technical feasibility of repeated PIPAC procedures. Secondary endpoints included perioperative outcomes, repeatability of laparoscopic access, postoperative complications, and reasons for treatment interruption.
Complications were graded according to the Dindo–Clavien classification.
Results
Between December 2024 and December 2025, 24 PIPAC procedures were performed in 10 patients with peritoneal metastases from ovarian and gastrointestinal malignancies.
The number of procedures per patient ranged from 1 to 6. PCI at first PIPAC frequently exceeded 15 and reached values greater than 20 in several patients.
Clinical characteristics and procedural outcomes are summarized in Table 1.
Clinical characteristics and procedural outcomes of patients treated with repeated PIPAC
| Patient | Age | Primary tumor | PCI at first PIPAC | No. of PIPAC procedures | Completed ≥3 cycles | Main clinical findings | Technical difficulties | Reason for treatment discontinuation | Major complications |
|---|---|---|---|---|---|---|---|---|---|
| A | 66 | High-grade serous ovarian carcinoma | >8 | 5 | Yes | Ascites resolution; marked reduction of peritoneal disease | Diffuse carcinomatosis | Ongoing treatment | None |
| B | 56 | High-grade serous ovarian carcinoma | >8 | 6 | Yes | Significant reduction of tumor burden; improved QoL | Adhesions during repeated access | Ongoing treatment | None |
| C | 80 | Borderline ovarian tumor | >15 | 2 | No | Stable residual disease; excellent tolerance | Hostile abdomen | Clinical deterioration and multidisciplinary reassessment | None |
| D | 55 | Colon adenocarcinoma | >25 | 2 | No | Partial stabilization of peritoneal disease; ascites improvement | Extensive carcinomatosis | Disease progression | None |
| E | 72 | Gastric carcinoma | >20 | 2 | No | Stable disease; symptomatic ascites control | Adhesions and diffuse disease | Worsening general clinical conditions | None |
| F | 66 | Pancreatic carcinoma | >15 | 2 | No | Stable peritoneal disease; symptomatic benefit | Hostile abdomen | Clinical deterioration | None |
| G | 61 | Appendix carcinoma | >20 | 1 | No | Limited assessment after first procedure | Diffuse carcinomatosis | Disease progression | None |
| H | 55 | Rectal carcinoma | >20 | 1 | No | Stable peritoneal involvement | Extensive adhesions | Clinical deterioration | None |
| I | 63 | Right colon adenocarcinoma | <6 | 1 | No | Limited disease control | Minimal adhesions | Multidisciplinary reassessment | None |
| J | 59 | Gastric carcinoma | >8 | 2 | No | Stable disease after repeated PIPAC | Diffuse peritoneal disease | Disease progression | None |
QoL, quality of life.
Despite diffuse carcinomatosis and previous systemic treatments, laparoscopic abdominal access was achieved in all procedures without conversion to laparotomy. Repeated PIPAC cycles remained technically feasible even in patients with hostile abdomens and extensive peritoneal disease.
Trocar positioning and access strategy were adapted according to intra-abdominal findings and adhesions. Previous trocar sites were preferentially reused during repeated procedures. Limited adhesiolysis using cold scissors was occasionally required to safely obtain adequate working space.
Mean operative time was 96 min and mean postoperative hospital stay was 1.2 days. No intraoperative complications occurred, and no major postoperative complications (Dindo–Clavien ≥III) were observed.
Treatment interruption in patients undergoing fewer than three procedures was mainly related to disease progression, worsening general clinical conditions, or multidisciplinary reassessment rather than technical impossibility of the procedure itself.
Representative intraoperative findings are shown in Fig. 1, demonstrating diffuse carcinomatosis, hostile abdominal conditions, and technical feasibility of repeated PIPAC procedures.
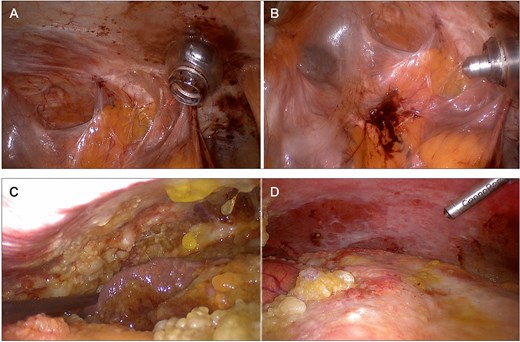
Technical feasibility of repeated PIPAC in hostile abdomen. (A) Extensive intra-abdominal adhesions and difficult laparoscopic field during repeated PIPAC. (B) Despite diffuse adhesions and limited working space, correct positioning of the CapnoPen® device allowed safe aerosol chemotherapy administration. Repeated PIPAC in diffuse peritoneal carcinomatosis. (C) Diffuse peritoneal carcinomatosis with ascites and extensive peritoneal involvement during exploratory laparoscopy. (D) CapnoPen® positioning and aerosol delivery remained feasible despite advanced peritoneal disease and hostile abdominal conditions.
Discussion
The present study describes the technical feasibility and reproducibility of repeated PIPAC procedures in patients with advanced peritoneal metastases treated within a structured institutional pathway.
While several studies have reported the safety profile of PIPAC, limited attention has been dedicated to the practical surgical challenges associated with repeated laparoscopic access in patients with diffuse carcinomatosis and hostile abdomens [5, 6]. Our experience suggests that repeated procedures may remain technically achievable even in the presence of extensive disease burden and previous treatments.
Repeated laparoscopic access in patients with diffuse peritoneal metastases is often considered challenging because of adhesions, bowel distension, previous surgeries, and progressive carcinomatosis. In our experience, careful trocar planning, selective adhesiolysis, and individualized access strategies allowed safe completion of all procedures without conversion to laparotomy.
One of the most relevant findings of this series is that treatment interruption was predominantly related to oncologic progression and deterioration of general clinical conditions rather than inability to safely re-enter the abdomen. This observation may support the reproducibility of repeated PIPAC procedures when performed within a standardized multidisciplinary setting and may help clarify the practical limitations of PIPAC programs in real-world oncologic practice [7, 10].
No cases of technical failure in abdominal access or aerosol delivery were observed.
This observation may help clarify the practical limitations of repeated PIPAC programs in real-world oncologic practice.
Several technical aspects appeared particularly important in our experience. Individualized trocar positioning, reuse of previous access sites, cautious cold-scissor adhesiolysis, and targeted orientation of the CapnoPen® device contributed to maintaining procedural safety and reproducibility over multiple cycles [3, 8].
The use of a dedicated scope-holder arm and a high-pressure Medrad injector also facilitated stable aerosol administration and operative standardization.
Our study has several limitations, including its retrospective nature, small sample size, and heterogeneity of tumor types. Furthermore, the present analysis was not designed to evaluate oncologic efficacy or survival outcomes.
Nevertheless, this real-world experience highlights practical technical considerations that may be useful for centers implementing repeated PIPAC procedures in patients with advanced peritoneal metastases [11].
Conclusions
Repeated PIPAC procedures appear technically feasible and reproducible even in patients with advanced peritoneal metastases, hostile abdomens, and extensive carcinomatosis.
In our experience, treatment discontinuation was more frequently related to disease progression and deterioration of clinical conditions than to technical failure of abdominal access itself.
Careful multidisciplinary patient selection, individualized trocar positioning, cautious adhesiolysis, and procedural standardization appear essential to maintain safety and reproducibility over multiple treatment cycles.
Although limited by the retrospective design and small sample size, this real-world experience may provide useful practical information for centers implementing repeated PIPAC programs in routine surgical oncology practice.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}