





Abstract
Fish bone ingestion is common, but fish bone-induced gastric perforation is rare. Preoperative computed tomography (CT) may suggest fish bone-related lesions, although no foreign body may be identified intraoperatively in some cases. This report describes three patients with acute epigastric pain following recent fish consumption. CT showed gastric antral wall thickening and linear hyperdense shadows. All patients underwent emergency laparoscopic surgery, with two requiring conversion to open surgery. A fish bone was identified in one case, but no foreign body was identified in the other two cases. All patients underwent perforation repair, irrigation, and drainage, and no postoperative complications occurred. This case series highlights the importance of considering fish bone-induced gastric perforation in patients with acute epigastric pain and a recent history of fish consumption, emphasizing the diagnostic value of preoperative CT.
Introduction
Foreign body ingestion is a common clinical problem, with 80%–90% of cases resolving spontaneously, 10%–20% requiring endoscopic removal, and <1% necessitating surgery [1, 2]. Fish bone-induced gastric perforation most frequently occurs at anatomical narrowing sites such as the esophagus, terminal ileum, and colon, whereas involvement of the gastric antrum is relatively rare [3, 4]. The clinical presentation is often nonspecific, including abdominal pain, fever, and leukocytosis, and may mimic other acute abdominal conditions such as peptic ulcer perforation, cholecystitis, or appendicitis [5]. Furthermore, many patients do not recall foreign body ingestion, making early diagnosis challenging.
With advances in imaging, computed tomography (CT) has become essential for detecting fish bone-related complications, typically demonstrating linear hyperdense foreign bodies with surrounding inflammatory changes [6]. Surgical or endoscopic removal is generally recommended when perforation is suspected. However, in rare cases, despite strong radiological and clinical evidence, no foreign body is identified intraoperatively. The optimal management strategy in such situations—particularly whether aggressive exploration to locate the foreign body is warranted—remains unclear.
Here, we report three cases of suspected fish bone-induced gastric perforation, focusing on diagnostic challenges and surgical decision-making when no foreign body was identified intraoperatively.
Case 1
A 69-year-old man presented with dysphagia for 2 days, abdominal pain for 1 day, and acute exacerbation for 2 h following fish consumption. Initial symptoms included dysphagia and dull epigastric pain without nausea or vomiting. Physical examination revealed mild epigastric tenderness without rebound tenderness or guarding.
Laboratory tests showed a white blood cell count of 9.06 × 109/l with 76% neutrophils. Contrast-enhanced abdominal CT demonstrated a 3.7-cm linear hyperdense foreign body located between the inferior margin of the left hepatic lobe and the gastric antrum (Fig. 1A), with surrounding fat stranding, suggestive of fish bone-induced gastric perforation.
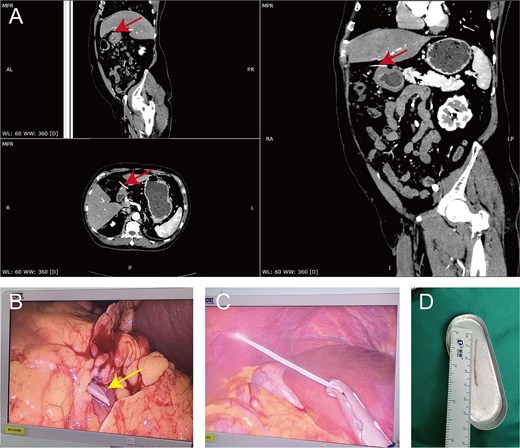
Preoperative imaging, intraoperative findings, and laparoscopic retrieval of the fish bone in Case 1. (A) Preoperative MPR CT of Case 1 revealed a 3.7 cm linear hyperdense foreign body (arrow) located between the inferior margin of the left hepatic lobe and the gastric antrum, associated with surrounding fat stranding, suggestive of localized inflammatory reaction. (B) Intraoperatively, a fish bone (arrow) was identified penetrating the serosal layer of the gastric antrum and was encapsulated by the greater omentum. (C) Fish bone retrieved via laparoscopy. (D) The fish bone measured ~3.7 cm in length using a ruler postoperatively. MPR, multiplanar reconstruction.
Laparoscopic exploration revealed a fish bone penetrating the serosal layer of the gastric antrum and encapsulated by the greater omentum (Fig. 1B–D). Local edema, hyperemia, and adhesions were noted, along with a firm sinus tract. No additional intra-abdominal injuries were identified. The foreign body was removed laparoscopically after for careful dissection and ligation of the surrounding omental tissue and sinus tract. The perforation was debrided and sutured, followed by abdominal irrigation and placement of drainage tubes in the subhepatic space and pelvis.
Postoperatively, the patient underwent fasting, gastrointestinal decompression, and a 1-week course of ceftriaxone. Inflammatory markers decreased significantly. A liquid diet was initiated on postoperative Day 7, drainage tubes were removed on Day 10, and the patient was discharged on Day 15 without complications. At 16-month follow-up, the patient remained asymptomatic, and repeat CT showed no abnormalities.
Case 2
A 65-year-old man presented with upper abdominal pain for 2 days, which had worsened over the preceding day, following ingestion of sea fish 3 days earlier. Physical examination revealed marked epigastric tenderness with mild guarding and rebound tenderness.
Laboratory tests showed a white blood cell count of 20.45 × 109/l, a neutrophil percentage of 88.2%, and an interleukin-6 level of 55.75 pg/ml. Contrast-enhanced abdominal CT demonstrated a small amount of pneumoperitoneum and exudative changes around the gastric antrum and pyloric region, with marked edema of the adjacent gastric wall. A 3.5-cm linear hyperdense shadow was also noted, suggesting fish bone-induced gastric antral perforation (Fig. 2A).
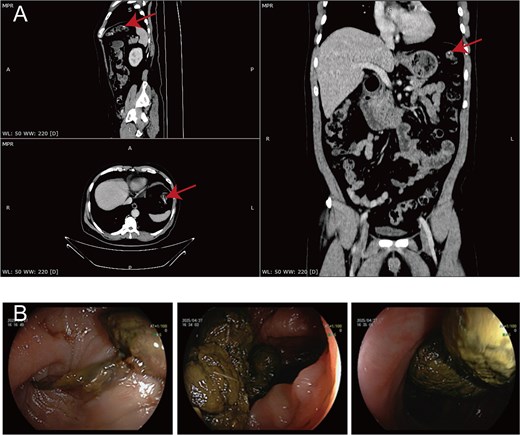
Preoperative CT and postoperative colonoscopic findings in Case 2. (A) Preoperative MPR CT of Case 2 showed a 3.5 cm linear hyperdense shadow (arrow) in the gastric antrum, accompanied by a small amount of free intraperitoneal gas and fluid collection around the gastric antrum and pyloric region, with marked adjacent gastric wall edema. (B) Postoperative colonoscopy showing no residual foreign body. MPR, multiplanar reconstruction.
Laparoscopic exploration identified an ~0.2-cm perforation on the posterior wall of the stomach with minor leakage of gastric contents. Surrounding peritoneal edema and hyperemia were present; however, no foreign body was detected. Because of limited exposure and difficulty with suturing, conversion to open surgery was performed to repair the posterior wall perforation. Intraoperative re-exploration failed to identify the fish bone. The abdominal cavity was irrigated thoroughly, and drainage tubes were placed in the subhepatic and pelvic spaces fish bone.
Postoperatively, the patient underwent fasting, gastrointestinal decompression, and ceftriaxone therapy. The peak body temperature reached 39.1°C but gradually normalized after 10 days of treatment, along with improvement in inflammatory markers. Colonoscopy on postoperative Day 2 showed no mucosal abnormalities, suggesting spontaneous passage of the fish bone (Fig. 2B). A liquid diet was initiated and drainage tubes were removed on postoperative Day 10, and the patient was discharged on Day 12. At 6-month follow-up, the patient remained asymptomatic without recurrence.
Case 3
A 77-year-old woman presented with acute upper abdominal pain for more than 3 h shortly after consuming fish. The pain was severe and associated with tenderness, rebound tenderness, and mild guarding, without fever or vomiting.
Laboratory tests revealed a white blood cell count of 15.24 × 109/l with 88.8% neutrophils. Contrast-enhanced abdominal CT demonstrated an ~3.0-cm linear hyperdense shadow extending from the anterior gastric wall to the right upper abdomen, with surrounding fat stranding, suggestive of fish bone-induced gastric perforation (Fig. 3A). Plain abdominal radiography showed no intestinal dilation or air–fluid levels but identified corresponding high-density shadows.
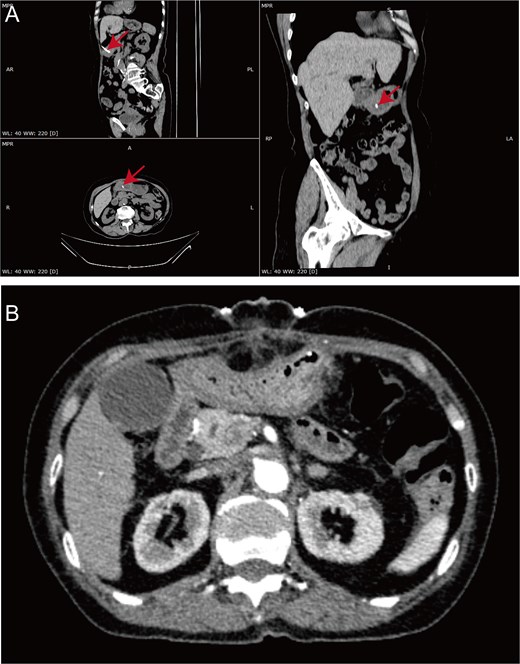
Preoperative and postoperative CT findings in Case 3. (A) Preoperative MPR CT of Case 3 demonstrated an ~3.0 cm linear hyperdense shadow (arrow) extending from the anterior wall of the stomach to the right upper abdomen, associated with surrounding fat stranding. (B) Postoperative CT demonstrated no evidence of the previously observed 3.0 cm linear hyperdense shadow, indicating resolution of the lesion. MPR, multiplanar reconstruction.
Laparoscopic exploration revealed an ~1-mm perforation on the anterior wall of the gastric antrum with localized exudation and mild omental adhesions. No foreign body was identified despite thorough exploration, prompting conversion to open surgery. Intraoperative re-exploration of the gastric wall, omentum, and abdominal cavity remained negative, and intraoperative radiography failed to detect any foreign body. Intraoperative gastroscopy demonstrated mucosal congestion, edema, and superficial erosion of the gastric antrum without a visible intraluminal foreign body. The perforation was repaired, and the patient’s family was informed of the potential risk of missed foreign body and re-perforation.
Postoperatively, the patient underwent fasting, gastrointestinal decompression, and ceftriaxone therapy for ~1 week. Inflammatory markers decreased significantly. Follow-up CT on postoperative Day 5 showed resolution of the previously observed hyperdense shadow and improvement in local inflammation (Fig. 3B). A liquid diet was initiated on postoperative Day 9, and the drainage tube was removed on Day 12, with discharge on the same day. At 1-year follow-up, the patient remained asymptomatic without recurrence.
Discussion
Fish bones are among the most commonly ingested foreign bodies, particularly in high-risk groups such as children, denture wearers, and individuals with impaired cognition [7, 8]. Due to their sharp structure, they can cause mucosal injury and, in rare cases, complications including abscess, obstruction, bleeding, and perforation [9]. Perforation typically occurs at sites of physiological narrowing or angulation, most commonly in the esophagus, small intestine, and colon, whereas gastric involvement—especially in the antrum—is relatively uncommon [10, 11].
The clinical presentation is often nonspecific. Abdominal pain is the most frequent symptom, followed by fever and leukocytosis, and the condition can easily be misdiagnosed as other causes of acute abdomen [12]. Although perforation occurs in <1% of cases, associated mortality can reach 9.6% due to sepsis [13]. Importantly, many patients do not recall foreign body ingestion [14]. In our series, all patients reported recent fish consumption, highlighting the importance of targeted history-taking in patients with unexplained upper abdominal pain.
CT is the preferred imaging modality for suspected fish bone-related perforation, typically demonstrating a linear hyperdense structure with surrounding inflammatory changes [15, 16]. It provides valuable information regarding the location of the foreign body and associated complications. However, its diagnostic accuracy may be influenced by factors such as slice thickness, foreign body orientation, and surrounding inflammation [17]. Therefore, CT findings should always be interpreted in conjunction with the clinical presentation.
In our series, all three patients had CT findings suggestive of fish bone-induced gastric perforation, yet the foreign body was identified intraoperatively in only one case. Several mechanisms may explain this discrepancy. First, spontaneous passage of the fish bone through the gastrointestinal tract after perforation cannot be completely excluded, which may leave only localized inflammatory changes at the perforation site [18]. Second, small or fragile fragments may be degraded or encapsulated by omental and fibrous tissue, rendering them undetectable. Third, linear hyperdense lesions on CT imaging may occasionally represent false-positive findings rather than true fish bones. Potential mimickers include vascular calcifications, ingested hyperdense materials, inflammatory strands, fibrotic tissue, and imaging artifacts. In addition, surrounding inflammatory changes may obscure the actual nature and precise location of the suspected foreign body. Previous studies have reported that the diagnostic accuracy of CT may be affected by several factors, including slice thickness, the orientation of the foreign body, the use of contrast agents, and the experience of the interpreting radiologist. In some cases, fish bones may even be misinterpreted as small vascular structures on CT imaging [18–20]. These findings emphasize the limitations of relying solely on imaging.
Previous reports have mainly described cases in which the fish bone was identified intraoperatively or endoscopically. In contrast, two patients in our series had CT findings highly suggestive of fish bone-induced gastric perforation, but no foreign body was identified during surgery. Therefore, the main novelty of this case series lies in its focus on this CT-positive but surgery-negative scenario, which may represent spontaneous passage of the fish bone or possible false-positive CT findings, as discussed above. Based on this observation, we propose a practical intraoperative strategy: when no foreign body is identified despite careful exploration, perforation repair, adequate peritoneal lavage, and drainage should be prioritized over exhaustive or blind exploration for the fish bone. In Cases 2 and 3, because of severe local inflammation and limited laparoscopic visualization, the fish bone was difficult to detect laparoscopically. Therefore, during the surgery, we converted to open abdominal surgery to complete the perforation repair. Although laparoscopic repair may be technically feasible, conversion to open surgery can provide better exposure and facilitate secure closure when inflammation is severe or the lesion is difficult to access. Intraoperative endoscopy, radiography, or ultrasound may be considered as adjunctive tools when localization of the foreign body remains uncertain. This strategy may help reduce unnecessary exploration and procedure-related risks [21]. Postoperative confirmation may subsequently be achieved by CT imaging or endoscopic examination [22]. This approach may provide a practical and feasible management strategy for similar cases in which preoperative CT strongly suggests fish bone-induced gastric perforation, but no foreign body is identified during surgery. Based on these findings, we developed a practical clinical management algorithm for suspected fish bone-induced gastric perforation (Fig. 4). Furthermore, it may help reduce operative time and minimize procedure-related complications. The primary therapeutic goals should be timely perforation repair and effective infection control. Laparoscopic exploration is recommended as the initial approach, with conversion to open surgery when necessary, particularly for posterior gastric lesions [23, 24]. Regardless of whether the foreign body is identified, priority should be given to perforation repair, adequate peritoneal lavage, and drainage. Adjunctive postoperative evaluation with CT or endoscopy may help exclude retained foreign bodies. In our cases, a strategy of “perforation repair plus infection control” resulted in favorable outcomes without recurrence or major complications.
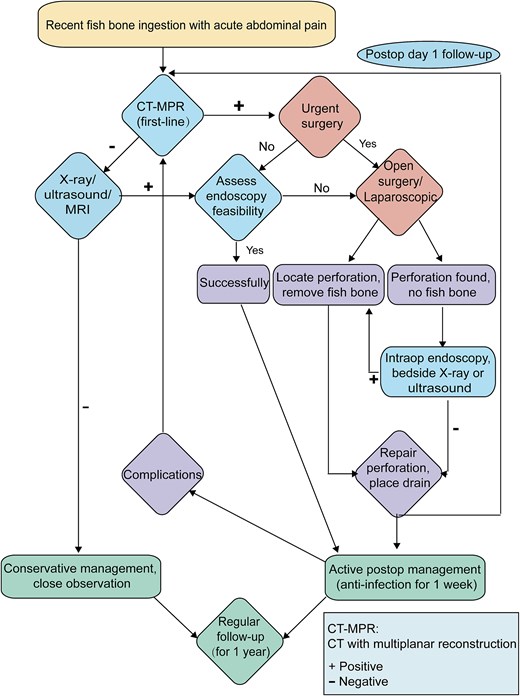
Clinical management algorithm for patients with suspected fish bone ingestion presenting with abdominal symptoms.
In conclusion, fish bone-induced gastric perforation is rare and often difficult to diagnose. When CT findings strongly suggest perforation but no foreign body is identified intraoperatively, surgical management should prioritize treatment of the perforation rather than exhaustive attempts to locate the foreign body. An individualized approach balancing surgical invasiveness and diagnostic certainty is essential.
Acknowledgements
The authors thank the Department of Radiology at Guangzhou Red Cross Hospital for their assistance in image acquisition.
Author contributions
Liansheng Mai designed and supervised the study, collected the clinical data, and drafted the manuscript. Qiguang Zhong, Hanshuo Zhang, Tang Chenyao and Shaojie Liu assisted in data organization and manuscript revision. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
This work was financially supported by the research grants of Guangzhou Municipal Science and Technology Bureau (Grant Number 2024A03J0673).
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary files. No additional datasets were generated or analyzed.
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Guangzhou Red Cross Hospital. Written informed consent for participation was obtained from all patients prior to publication.
Consent for publication
Written informed consent was obtained from all patients for publication of this case series and any accompanying clinical images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}