





Abstract
Bowel obstruction caused by ingestion of water-absorbing beads is an increasingly recognized pediatric emergency. We report four cases in children under 5 years of age presenting with bilious vomiting and absence of bowel movements. Plain radiographs demonstrated features of small bowel obstruction without visualization of the foreign body, while ultrasound revealed cystic intraluminal lesions suggestive of obstruction. Surgical exploration confirmed expanded beads causing complete intestinal obstruction at different levels of the small intestine. Enterotomy with foreign body removal and bowel repair was performed in all patients, with uneventful recovery. No additional beads were identified intraoperatively, and no recurrent bowel obstruction was observed during at least 3 months of follow-up. Water-absorbing beads pose a unique diagnostic challenge because they are radiolucent and may mimic gastroenteritis. Their ability to expand after passing the pylorus can result in delayed complete obstruction. Early recognition and timely surgical intervention are essential to prevent serious complications.
Introduction
Water beads are small colorful spheres composed of superabsorbent polymers, commonly sodium polyacrylate or polyacrylamide, marketed as children’s sensory toys, floral decorations, and toy gun projectiles [1, 2]. In their dry state, they measure 1–5 mm in diameter but can expand up to 150–1500 times their original volume after fluid exposure [2]. Because they are not readily biodegradable, they may persist and enlarge within the gastrointestinal tract [2]. Ingestion is the most dangerous form of injury, particularly in children under 5 years of age [1, 3]. Expansion of the beads may cause life-threatening bowel obstruction [1, 2]. Diagnosis is often delayed because the beads are radiolucent and difficult to detect on plain radiographs, requiring ultrasound or computed tomography (CT) scans for localization [1, 4–6]. Symptoms are nonspecific and may mimic gastroenteritis [1]. Surgical intervention is usually required for complete obstruction [1, 2, 5].
We report four cases of bowel obstruction caused by water-absorbing bead ingestion and discuss their clinical presentation, imaging findings, operative management, and outcomes in accordance with the PROCESS 2025 criteria [7].
Case series
All operations were performed by board-certified pediatric surgeons with more than 10 years of experience in pediatric gastrointestinal surgery. A limited open abdominal approach was used. After identification of the transition zone, a longitudinal enterotomy was made on the antimesenteric border at or near the obstructing bead. The foreign body was removed, the remaining bowel was carefully examined and milked to exclude additional beads, and the enterotomy was closed transversely using interrupted absorbable sutures.
Case 1
A 20-month-old female was admitted with a 3-day history of vomiting. After returning from daycare, she consumed candies of unknown type and subsequently developed vomiting without fever or bowel movements. She was initially treated at a private clinic for presumed gastrointestinal infection. On Day 3, persistent vomiting of food and yellow fluid, decreased oral intake, fatigue, and constipation prompted hospital admission. She was initially diagnosed with suspected gastroenteritis and treated with antibiotics, intravenous fluids, digestive enzymes, and laboratory investigations. During hospitalization, she developed colicky abdominal pain, bilious vomiting, and persistent constipation. Physical examination revealed a soft mildly distended abdomen without localized tenderness. Ultrasound demonstrated two round anechoic intraluminal lesions measuring ~28 × 28 mm, associated with dilated fluid-filled small bowel loops (Fig. 1). Abdominal X-ray showed dilated bowel loops without radiopaque foreign bodies (Fig. 1). She was transferred for surgical evaluation because of suspected intestinal obstruction caused by a gastrointestinal foreign body. Differential diagnoses included phytobezoar, intraluminal polyps, and duplication cysts. Surgery revealed a transition zone 30 cm distal to the ligament of Treitz containing a foreign body. Jejunotomy was performed to remove a 4 cm expanded bead. Another bead located in the third portion of the duodenum was milked to the enterotomy site and removed. The bowel was sutured. Postoperative recovery was uneventful, oral feeding resumed on postoperative Day 2, and the patient was discharged on postoperative Day 8.
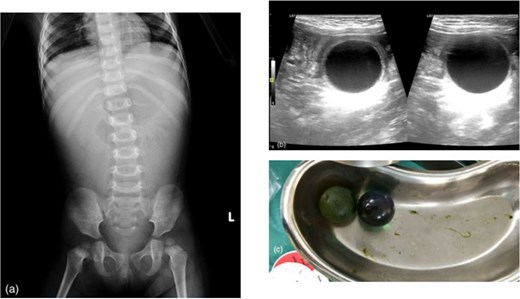
(a) Abdominal X-ray showing dilated bowel loops, (b) ultrasound images revealing two spherical anechoic lesions, (c) intraoperative findings revealing two water-absorbing beads.
Case 2
A 21-month-old male presented with a 2-day history of vomiting of food mixed with yellow fluid, without fever or bowel movements. Past history was unremarkable. He continued to vomit, and nasogastric tube drainage showed green fluid. Physical examination revealed constipation and a soft moderately distended abdomen. Abdominal ultrasound demonstrated multiple dilated small bowel loops (~21 mm) with increased peristalsis and a 27 × 27 mm thin-walled cystic intraluminal lesion in the lower abdomen (Fig. 2). Abdominal X-ray showed multiple dilated bowel loops with uneven gas distribution, without definite air-fluid levels or radiopaque foreign bodies (Fig. 2). He was diagnosed with suspected intestinal obstruction due to a foreign body, with differential diagnoses including phytobezoar, intraluminal polyps, and duplication cysts. Surgery revealed uniformly dilated small bowel loops from the ligament of Treitz to ~30 cm proximal to the ileocecal valve. A 3 × 3 cm expanded bead causing complete ileal obstruction was identified, with collapse of the distal ileum and colon. Enterotomy with foreign body removal, bowel milking, and closure was performed. Postoperative recovery was uneventful, oral feeding resumed on postoperative Day 2, and the patient was discharged on postoperative Day 7.
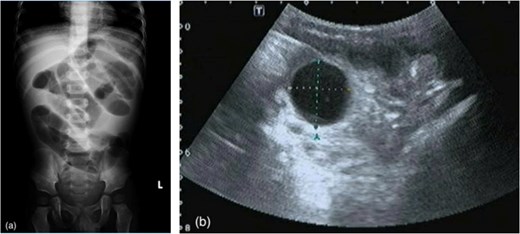
(a) Abdominal X-ray showing dilated bowel loops, (b) ultrasound images revealing a spherical anechoic lesion measuring 27 × 27 mm.
Case 3
A 16-month-old female was admitted for vomiting. The illness had lasted 2 days, characterized by frequent vomiting of food and yellow fluid, no fever, no bowel movements, and decreased oral intake. Past history was unremarkable. She continued to vomit, and nasogastric tube drainage showed green fluid. Physical examination revealed constipation and a soft moderately distended abdomen. Abdominal ultrasound demonstrated multiple dilated fluid-filled small bowel loops with increased peristalsis and a 25 × 20 mm cystic lesion in the left lower abdomen, with differential diagnoses including intestinal obstruction, mesenteric cyst, or ovarian cyst (Fig. 3). Abdominal X-ray showed dilated bowel loops with paucity of distal gas, without definite air-fluid levels or radiopaque foreign bodies, suggestive of intestinal obstruction (Fig. 3). She underwent surgery for intestinal obstruction, with differential diagnoses including phytobezoar, intraluminal polyps, and duplication cysts. Intra-operatively, markedly dilated small bowel loops and clear yellow fluid in the Douglas pouch were noted. A transition zone 40 cm proximal to the ileocecal valve contained a slightly mobile foreign body. Enterotomy revealed an expanded bead measuring ~2 × 2 cm, which was removed (Fig. 3). The bowel was milked and sutured. Postoperative recovery was uneventful, oral feeding resumed on postoperative Day 2, and she was discharged on postoperative Day 7.
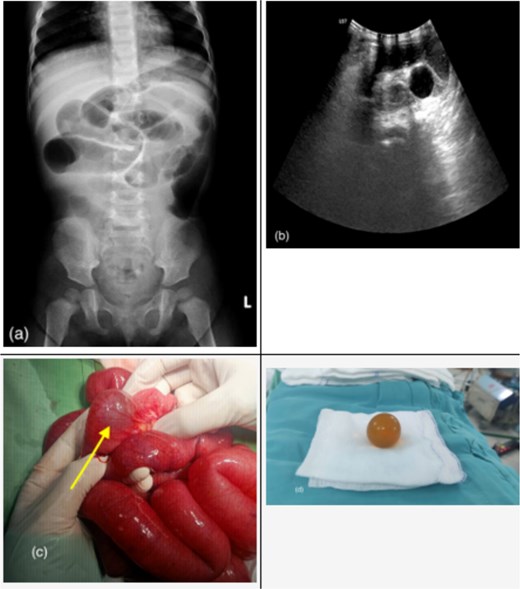
(a) Abdominal X-ray showing dilated bowel loops, (b) ultrasound images revealing a spherical anechoic lesion, (c) intraoperative findings revealing an intraluminal foreign body (arrow), (d) extracted 20 × 20 mm water-absorbing bead.
Case 4
A 25-month-old boy presented with a 1-day history of recurrent vomiting, intermittent abdominal pain, and failure to pass stool. Past history was unremarkable. Physical examination revealed moderate abdominal distension without palpable mass or signs of peritonitis. Abdominal ultrasound demonstrated a cystic lesion in the right upper abdomen with dilated proximal bowel loops and collapsed distal bowel loops, suggestive of intestinal obstruction secondary to an enteric duplication cyst. Abdominal X-ray showed dilated bowel loops with paucity of distal bowel gas. Differential diagnoses included enteric duplication cyst, phytobezoar, and intraluminal foreign body. Emergency laparoscopy revealed dilated small bowel loops and a transition point in the ileum ~20 cm proximal to the ileocecal valve containing a smooth intraluminal foreign body. The umbilical incision was extended, and enterotomy was performed to remove a 2 × 2 cm spherical expandable bead. No additional foreign bodies were identified, and the enterotomy was closed. Postoperative recovery was uneventful, oral feeding resumed on postoperative Day 2, and the patient was discharged on postoperative Day 8 without complications.
All four patients were followed for a minimum of 3 months after surgery. During this period, they tolerated normal feeding, had regular bowel movements, and showed no evidence of recurrent bowel obstruction or wound-related complications.
Discussion
Bowel obstruction caused by water-absorbing beads (water beads or jelly beads) is an increasingly recognized pediatric emergency associated with diagnostic challenges. These super-absorbent polymer beads can expand from 1 to 5 mm to 150–1500 times their original volume after contact with digestive fluids, leading to mechanical obstruction at narrow points of the gastrointestinal tract [2, 8]. National data from the USA estimated 8159 water bead-related emergency department visits between 2007 and 2022, with cases increasing by over 130% from 2021 to 2022 [1]. Children under 5 years are most commonly affected [1]. Notably, all patients in our series were 25 months of age or younger. Clinical manifestations are nonspecific and often mimic gastroenteritis, with vomiting being the most common symptom [1, 4, 8]. Diagnosis is difficult because the beads are radiolucent and rarely visible on plain radiographs [1, 5, 8]. Ultrasound commonly demonstrates anechoic spherical lesions, whereas CT scans may identify intraluminal masses with clear margins [5, 8]. In our series, ultrasound was the most useful preoperative imaging modality, while CT was not performed because all patients had clinical and sonographic evidence of complete obstruction requiring surgery. Water-absorbing beads may continue to enlarge after imaging because of ongoing absorption of intestinal fluid, which may explain the difference between ultrasonographic and intraoperative measurements. All four patients underwent enterotomy with foreign body removal and bowel repair without postoperative complications or retained foreign bodies. Previous reports have described severe complications including repeat laparotomy, anastomotic leakage, septicemia, and death [2, 9]. Endoscopic removal may be effective for proximal beads, while conservative management has been reported in selected asymptomatic or older patients [2, 4, 5, 9]. Osmotic laxatives should be avoided because they may promote further bead expansion [6, 9]. The main strength of this case series is the description of a consistent clinical pattern in four young children with surgically confirmed bowel obstruction caused by water-absorbing beads. However, the study is limited by the small sample size, retrospective single-center design, limited follow-up, and absence of CT evaluation.
Conclusion
Water-absorbing bead ingestion should be considered in young children presenting with unexplained vomiting and signs of bowel obstruction. Early diagnosis and timely surgical intervention are essential to prevent severe complications.
Author contributions
H.T.B. contributed to study conception and design, patient management, data collection, literature review, manuscript drafting, and manuscript revision. T.T.T., N.H.N.P. and Q.T.V.H. contributed to patient care, critical revision of the manuscript, and supervision. All authors read and approved the final manuscript.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
None declared.
Consent for publication
Written informed consent was obtained from the parents or legal guardians of all patients included in this case series for publication of this article and any accompanying images. Copies of the written consents are available for review by the Editor-in-Chief of this journal.
References
Lei H, Yang J, Bian H et al. . Superabsorbent polymer beads ingestion by children: a single-center retrospective study of 11 cases. BMC Pediatr 2026;

{kind=link}
{kind=link}
{kind=link}