





Abstract
Pyelo-digestive fistulas are exceptional clinical entities. We report an extremely rare communication between the renal pelvis of an ectopic pelvic kidney and the sigmoid colon, representing only the second such case documented in the global literature. A 45-year-old male presented with recurrent urinary tract infections and abdominal pain. Excretory-phase computed tomography revealed a left pelvic ectopic kidney with pneumopyelia and a direct fistulous tract to the sigmoid colon. A multidisciplinary approach was performed, consisting of a segmental sigmoid resection with primary anastomosis, combined with a conservative reduction pyeloplasty. Postoperative recovery was uneventful, and the 12-month follow-up showed no recurrence. Unlike classic pyelo-colic fistulas, pelvic ectopy facilitates direct contact with the sigmoid colon due to altered anatomical relationships. This case demonstrates that conservative multidisciplinary surgery is a viable alternative to radical nephrectomy when renal function is preserved. Awareness of this variant is essential to avoid diagnostic pitfalls.
Introduction
Uro-digestive fistulas are defined as abnormal communications between the urinary tract and the gastrointestinal tract. Although relatively rare overall, their incidence varies according to anatomical location. Vesico-digestive fistulas represent the most frequent forms; however, fistulas involving the upper urinary tract remain exceptional. Etiologies are diverse, primarily dominated by traumatic or infectious origins, while spontaneous cases are extremely rare. Management remains challenging and often requires a multidisciplinary approach involving urologists, visceral surgeons, and radiologists. We report a rare case of a pyelo-sigmoid fistula in a pelvic ectopic kidney and discuss the diagnostic and therapeutic aspects. To our knowledge, following a global literature review, this represents only the second documented case of spontaneous communication between the renal pelvis of a pelvic ectopic kidney and the sigmoid colon.
Case presentation
We report the case of a 45-year-old male with a lifelong history of intellectual disability and no notable surgical history. He was admitted for recurrent urinary tract infections (UTIs) associated with diffuse abdominal pain and digestive problems persisting for several weeks. Clinical examination revealed a febrile patient (38.5°C), with left lumbar tenderness radiating to the hypogastric region and no deterioration of general status. Laboratory findings showed an inflammatory syndrome with leukocytosis and elevated C-reactive protein (CRP), while urine culture identified an infection with Enterococcus faecium.
Abdominopelvic computed tomography (CT) with contrast injection and excretory phase demonstrated left pyelocaliceal dilatation in a malrotated pelvic kidney. Imaging also revealed pneumopyelia within the left renal collecting system and a fistulous communication between the renal pelvis and the sigmoid colon (Fig. 1).
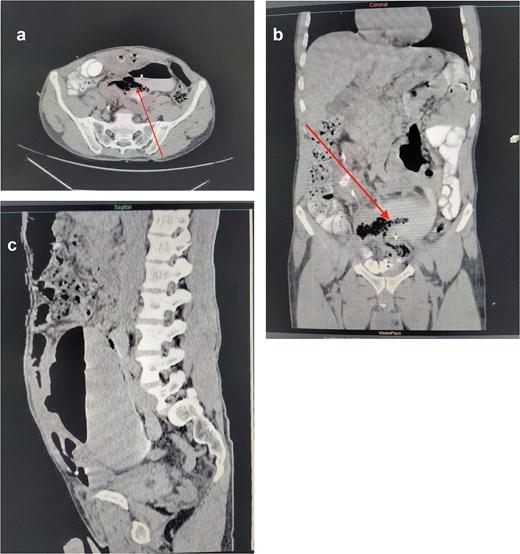
Preoperative imaging: Contrast-enhanced abdominal and pelvic CT scan [axial (a), coronal (b), and sagittal (c) sections]. The image shows an ectopic left renal pelvis with significant pyelocaliceal dilatation. There is air present in the renal cavities (pneumopyelia) and a direct fistulous tract (arrow) between the renal pelvis and the sigmoid colon.
Given the predominant infectious context, the patient was started on broad-spectrum antibiotic therapy (third-generation cephalosporin, aminoglycoside, and metronidazole). Endoscopic drainage of the left kidney was performed using a simple ureteral stent. This allowed for the exteriorization of fecaluria, confirming the diagnosis of a high uro-digestive fistula.
Following stabilization of the infectious status, surgery was indicated. The procedure was performed via an open midline laparotomy. Intraoperative exploration revealed significant inflammatory adhesions in the ileal loops, as well as between the left renal pelvis and the sigmoid colon, with the fistula tract being identified (Fig. 2a–c). A conservative surgical strategy was chosen, consisting of a segmental resection of the sigmoid colon including the fistulous tract, with primary colo-colic anastomosis, following thorough lavage and cleaning of the renal sinuses, a reduction pyeloplasty was performed (using the Anderson-Hynes technique) (Fig. 2), with a double-J stent inserted. Figure 3 shows the solid specimen after fixation in formalin at the histology laboratory.
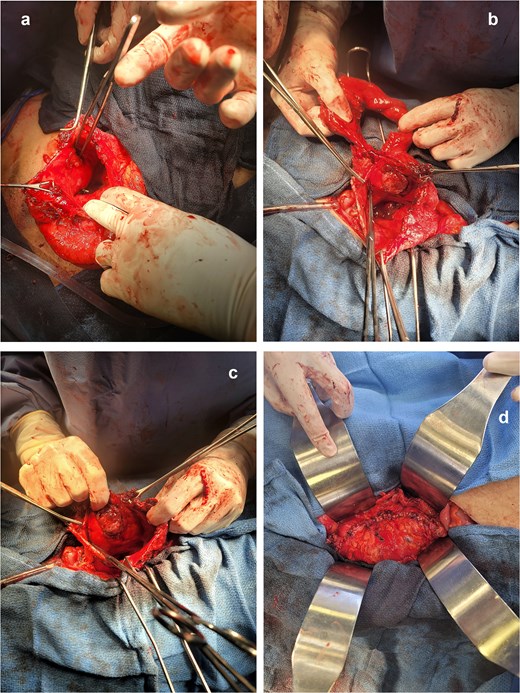
Intraoperative views via median laparotomy. (a–c) Examination of the collecting system following pyelotomy. The renal pelvis is widely open, revealing the ureteral catheter in place. The opening of the pyelo-sigmoid fistula (indicated by the arrow) connecting the renal cavity with the lumen of the sigmoid colon is clearly visible. (d) Reconstruction phase. Final view following segmental resection of the sigmoid colon (colo-colic anastomosis not visible here) and performance of a reduction pyeloplasty. Continuity of the upper urinary tract is restored via a double-J stent.
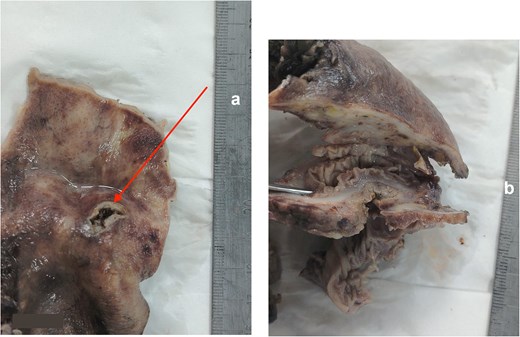
Single-piece resection specimen (colonic segment and pyelic wall) following fixation in formalin. (a) Intra-pyelic view of the fistula. The opening of the renal pelvis reveals the fistulous orifice (arrow) within an inflamed and remodeled pyelic mucosa, indicating chronic passage of digestive contents into the upper urinary tract. (b) View following sectioning of the fistulous tract. This cross-section of the tract highlights the direct communication between the colonic wall and the wall of the renal pelvis. Note the thickness of the peri-fistular inflammatory remodeling that connects the two organs.
The post-operative course was uneventful, with symptoms resolving and bowel movements resuming on day 3; the double-J stent was removed at 3 months. Follow-up at 12 months showed no evidence of recurrence.
Discussion
Pyelo-digestive fistulas are exceptional clinical entities, representing ~5% of all uro-digestive fistulas [1]. According to Goodwin’s rule, communications involving the upper urinary tract are predominantly of urological origin (kidney stones, chronic infections, or inflammation), however those in the lower tract are most often secondary to gastrointestinal pathology [2]. Although iatrogenic causes (cryoablation, and percutaneous nephrolithotomy) are increasingly reported.
The main feature of our observation lies in the association of a pelvic ectopic kidney with sigmoid colon participation. Classically, left pyelo-colic fistulas involve the descending colon or the left colonic angle due to the immediate proximity of the kidney in the lumbar position [3]. In our case, renal ectopia radically alters the anatomical relationships: the absence of protection by Gerota’s fascia and the pre-sacral position of the kidney promote direct contact with the mobile sigmoid colon. To date, after an exhaustive review of the global literature, this is only the second documented case of a pyelo-sigmoid fistula in an ectopic kidney [4]. The first reported case resulted in a nephrectomy; our observation is therefore notable for the success of a conservative strategy.
Clinical diagnosis is often delayed due to the non-specific nature of symptoms (abdominal pain, bowel disfunction), making the diagnosis complex and essentially dependent on the location of the tract [5]. However, the presence of faecaluria or pneumaturia, although rare in the upper urinary tract (unlike vesicocolic fistulas), is pathognomonic [6]. In our patient, the isolation of E. faecium in the urine was a strong indicator of a communication with the lower gastrointestinal tract.
Contrast-enhanced CT, particularly with delayed excretory phase imaging, constitutes the gold standard for investigation. It allows for a positive diagnosis by visualizing the passage of opacified urine into the colonic lumen, while assessing contralateral renal function and facilitating surgical planning [7]. The presence of pneumopyelia associated with a pelvic kidney should immediately raise suspicion of this entity. The CT scan may be supplemented by upper and lower gastrointestinal radiological examinations involving contrast.
The therapeutic strategy must be discussed on a case-by-case basis. Radical treatment (nephrectomy associated with colonic resection) is classically indicated in cases of a destroyed kidney, malignancy, or a frail patient [8].
However, our case demonstrates that a conservative treatment is feasible and safe when the renal parenchyma is functional. This choice relies on a triple requirement [9]:
(1) Rigorous infection control via targeted antibiotics and effective urinary drainage (double-J or ureteral stent),
(2) Complete excision of the fistulous tract through segmental colonic resection,
(3) Repair of the collecting system (reduction pyeloplasty) to treat the underlying cause (urinary stasis in a malrotated kidney).
The necessity of a diversionary stoma in inflammatory contexts remains controversial; although prudent in cases of peritonitis or malnutrition, it is not systematic following sepsis stabilization or in elective repairs. In our case, a primary colonic anastomosis without a diverting stoma was performed. This choice was justified by the absence of generalized stercoral peritonitis and good vascularization of the colonic margins, allowing for a reduction in overall morbidity and hospital stay [10].
This multidisciplinary approach, achieved complete healing without recurrence at 12 months, confirming the viability of conservative surgery for this extremely rare pathology.
Conclusion
Pyelo-sigmoid fistula is an exceptional clinical entity. Its diagnosis can be difficult due to non-specific symptomatology. Abdominopelvic CT remains the key diagnostic tool. Management is primarily surgical and can be complex due to local inflammatory processes. A multidisciplinary approach involving urologists and visceral surgeons is essential to achieve optimal outcomes.
Consent
Written informed consent was obtained from the patient’s legal guardian for the publication of this case report and any accompanying images.
The authors used [Gemini] to assist in the linguistic editing, translation from French to English, and structural organization of this manuscript to ensure academic standards. The final content was reviewed, verified, and edited by the authors, who take full responsibility for the clinical accuracy and integrity of the work.
Conflicts of interest
The authors declare no competing interests.
Funding
No funding was received for this study.

{kind=link}
{kind=link}
{kind=link}