





Abstract
Herniation through the foramen of Winslow is a rare internal hernia and an uncommon cause of intestinal obstruction. An 88-year-old man presented with epigastric pain, nausea, and vomiting for 2 days without previous abdominal surgery. Physical examination showed mild abdominal distension without peritoneal signs. Computed tomography demonstrated dilated small bowel loops within the lesser sac behind the stomach, suggesting herniation through the foramen of Winslow. Emergency laparotomy confirmed herniation of the ileum and cecum into the lesser sac. The bowel was congested but viable and was reduced without resection. Because of excessive mobility of the right colon, the cecum was fixed to the abdominal wall. The postoperative course was uneventful, and the patient was discharged in stable condition. Early diagnosis and prompt surgical intervention are essential for favorable outcomes.
Introduction
Internal hernias are an uncommon cause of intestinal obstruction, accounting for ˂1% of cases [1, 2]. Herniation through the foramen of Winslow is particularly rare, representing ~8% of internal hernias and ˂0.1% of all hernias [3]. This condition occurs when abdominal viscera protrude through the epiploic foramen into the lesser sac.
Predisposing factors include a long mesentery, failure of retroperitoneal fixation of the right colon, an enlarged foramen of Winslow, and sudden increases in intra-abdominal pressure [1, 4]. Clinical presentation is often nonspecific, making preoperative diagnosis difficult. Delayed treatment may lead to bowel strangulation, ischemia, or perforation.
Computed tomography (CT) has become the imaging modality of choice for diagnosing internal hernias, allowing early identification and timely surgical intervention [2]. We report a rare case of small bowel obstruction caused by herniation through the foramen of Winslow in an elderly patient successfully treated with emergency surgery.
Case report
An 88-year-old man presented with epigastric pain, nausea, and repeated vomiting for 2 days. He had no history of previous abdominal surgery. On examination, the abdomen was mildly distended with localized tenderness but without peritoneal signs. Vital signs were stable, and laboratory tests were within normal limits except for mild electrolyte imbalance.
Plain abdominal radiography and ultrasound were inconclusive. Contrast-enhanced CT demonstrated dilated small bowel loops measuring up to ~35 mm in diameter, containing both fluid and gas. The loops were located within the lesser sac behind the stomach, suggesting herniation through the foramen of Winslow (Fig. 1).
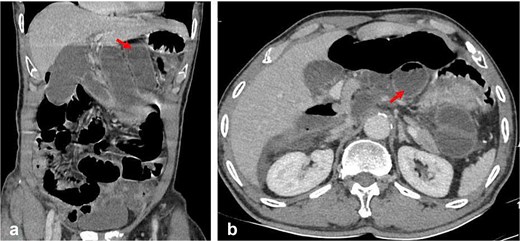
Contrast-enhanced CT images demonstrating herniation through the foramen of Winslow. (a) Coronal view showing dilated bowel loops (arrow) within the lesser sac posterior to the stomach. (b) Axial view demonstrating herniated bowel loops (arrow) located behind the stomach in the lesser sac.
Emergency laparotomy was performed. Intraoperatively, a segment of ileum along with the cecum was found herniating through the foramen of Winslow into the lesser sac (Fig. 2). The bowel appeared congested but viable, with no evidence of necrosis.
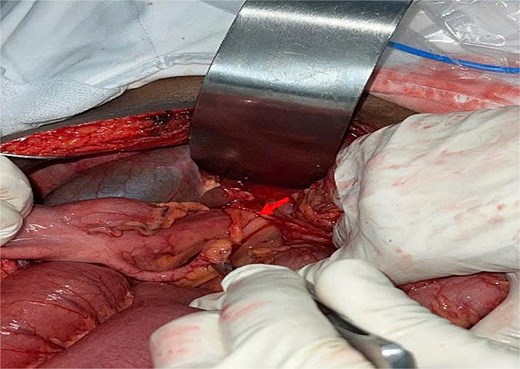
Intraoperative photograph demonstrating the herniated bowel passing through the foramen of Winslow (arrow). The herniated segment appears congested but viable.
Gentle reduction of the herniated bowel was achieved without difficulty. Bowel resection was not required. The foramen of Winslow was not closed due to the risk of injury to adjacent vascular structures, including the portal triad. Because the right colon was excessively mobile, the cecum was fixed to the abdominal wall to reduce the risk of recurrence.
The postoperative course was uneventful. Bowel function returned, oral intake was resumed, and the patient recovered without complications. He was discharged in stable condition.
Discussion
Herniation through the foramen of Winslow is a rare but potentially life-threatening condition [5]. It most commonly involves the small intestine, although the cecum, ascending colon, gallbladder, or omentum may also herniate [1, 3].
Clinical manifestations are nonspecific and typically resemble other causes of intestinal obstruction, making preoperative diagnosis difficult [2]. CT imaging plays a crucial role in diagnosis. Characteristic findings include bowel loops within the lesser sac, displacement of the stomach anteriorly, absence of bowel in the right lower quadrant, and mesenteric vessels passing between the portal vein and inferior vena cava [2].
Emergency surgery remains the definitive treatment. Reduction of the herniated bowel should be performed carefully to avoid injury to surrounding vascular structures. Bowel resection is required only if ischemia or necrosis is present [3, 6]. Closure of the foramen of Winslow is generally not recommended because of the proximity to the portal triad and the risk of vascular injury [6].
In this case, excessive mobility of the right colon likely contributed to the herniation, and cecal fixation was performed accordingly. Despite the patient’s advanced age, early diagnosis and prompt surgical intervention resulted in an excellent outcome.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}