





Abstract
The presence of a complex fistula is associated with a high recurrence rate. Lay-open technique with fistulotomy is imperatively contraindicated in cases of complex fistulas due to the 40% risk of early or delayed onset of anal incontinence. Combining different sphincter-preserving approaches aims to significantly reduce the chance of recurrence and preserve the quality of life. We present a case of a 34-year-old woman with a complex perianal fistula. We applied a combination of sphincter-sparing approaches by FiLAC, LIFT and TAFR. The follow-up period is 11 months without incontinence and recurrence. Despite the conflicting data published in the literature the combination of minimally invasive approaches for the treatment of secondary branches, interruption of the fistula tract, and thorough eradication of the internal opening of a highly complex fistula provides the greatest opportunity for achieving maximum success, i.e. minimizing the risk of recurrence while maintaining sphincter continence.
Introduction
The worldwide reported incidence of perianal fistula is 5.6/100 000 in women and 12.3/100 000 in men, with perianal fistulas occurring in 1.2–2.8 per 10 000 population in Europe [1]. The frequency distribution of fistula types varies in the literature [2–5]. Thus, the frequency of intersphincteric fistula is between 24% and 54%, transsphincteric between 30% and 58% and suprasphincteric between 1% and 20%. The frequency of extrasphincteric fistulas is given as up to 5% in older publications [6] and up to 3% in more recent publications [7]. The term ‘Complex’ fistulas include those involving 30% or more of the external anal sphincter muscle mass, the presence of secondary tracts and cavities extending above the levator muscles, supra-levator or supra-sphincteric branches, horseshoe extensions, a history of Crohn's disease, cancer, previous surgery or radiotherapy, and pre-existing continence disorder [8]. The presence of a complex fistula is associated with a high recurrence rate (26%–36% vs. 1.3% for simple fistulas; P < .001) [9, 10]. Due to the significant involvement of the external voluntary anal sphincter, the use of fistulotomy or fistulectomy (conventional for low/‘uncomplicated’ perianal fistulas) is strictly contraindicated for high complex fistulas unless combined with a single-stage, primary sphincter reconstruction, which is also fraught with serious debatability in terms of analysis of published data. Еncouraging clinical data exist for the increasingly established other sphincter-sparing surgical methods. Regardless of the chosen approach, all serious literature data indicate a maximum success rate for complex fistulas within 65%–73% at 5-year follow-up. One of the most pivotal moments in the different surgical approaches is the achievement of adequate ‘closure’, i.e. elimination of the internal opening of the fistula tract [11]. In certain clinical cases, the combination of two or more sphincter-preserving approaches in complex fistulas would carry the presumption that this would increase the success rate, respectively—reduce the recurrence rate.
Case report
We report a case of a 34-year-old woman with a complex perianal fistula. About 3 months after the appearance of an external opening of the anoderm at 1 o'clock in the lithotomy position, presenting with episodic leakage of purulent exudate, a perianal fistula was noted. This necessitated conducting an endoanal ultrasound (EAU) (Fig. 1), through which we found: a main fistula course crossing the external anal sphincter at the border of the middle/upper third of the length of the anal canal with a direction towards the external opening, as well as a secondary dorsal extension.
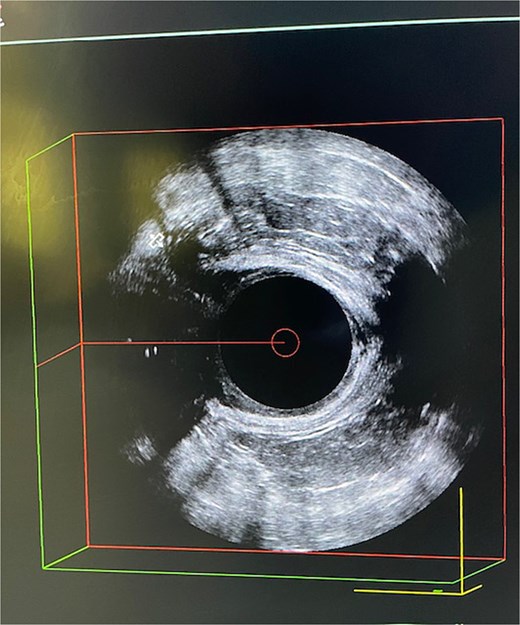
EAU with two extensions of the complex perianal fistula.
These ultrasonographic findings classified the fistula as ‘complex’—Grade IV according to Garg [12]. At this stage, we placed a ‘loose’ seton (Fig. 2) along the main fistula tract in order to ensure permanent drainage of the existing intersphincteric sepsis.
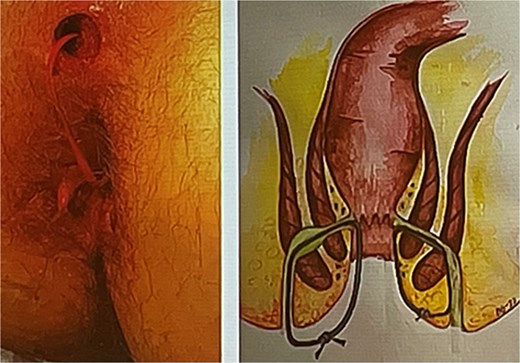
Loose seton as preparation for definitive treatment (left)—own case; (right)—schematic representation.
The presence of such a degree of ‘complexity’ of a perianal fistula requires mandatory additional diagnostic imaging by magnetic resonance imaging (MRI) (Fig. 3a and b).
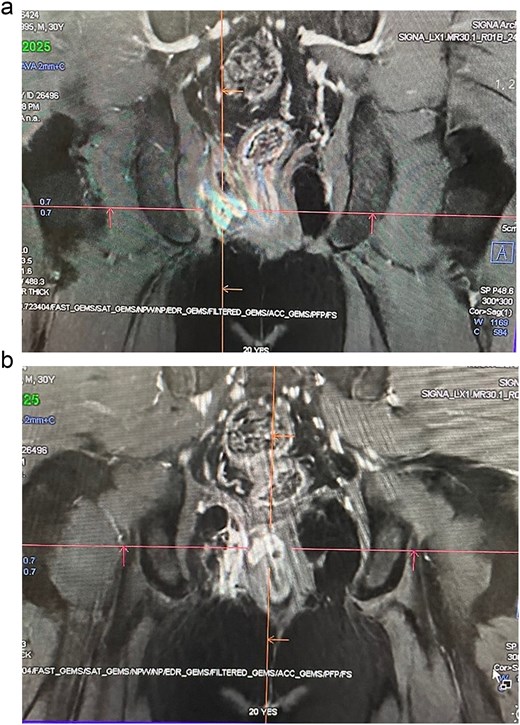
(a, b) MRI with contrast—H2O2–3% with visualization of the complex fistula with secondary extension.
The study confirmed the branched nature of the fistula. Due to the potentially significant risk of recurrence, we adopted the tactic of combining sphincter-preserving approaches in the surgical treatment in this particular case. The tactics we applied included conducting one stage of:
–Probing the fistula extensions with a soft ball-tip probe, then through it—passing a gauze strip along the fistula passages and debridement of the lumen/walls of the fistula tract (Fig. 4) with reciprocating ‘scraping’ movements of the gauze strip, then lavage of the lumen through the external opening with a 3% solution of hydroperoxide.
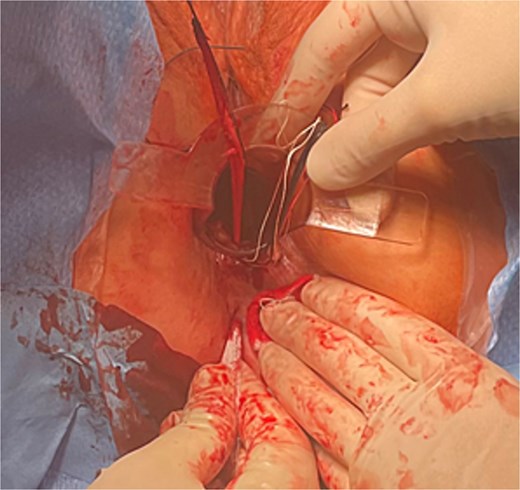
Debridement of a fistula tract with gauze tape.
–Application of laser ablation of the secondary fistula tract with a 360° fiber emitting light energy 1470ɳɱ, power 12 W, starting from the area of the internal opening in the direction distal to the external opening at a speed of 1 mm/s (Fig. 5a–d).
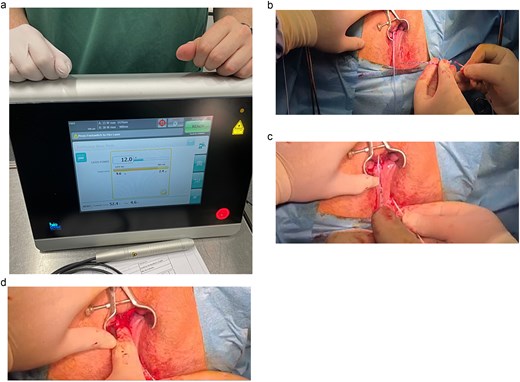
(a–d) Equipment used and sequential stages of performing the FiLAC procedure for dorsal fistula extension.
–Performance of LIFT—ligation of intersphincteric fistula tract (Fig. 6) through incision of the intersphincter groove, dissection of the intersphincter space, identification of the intersphincter segment of the main fistula tract before its branching, placement of two suture ligatures—PDS 2–0 at a distance of about 10 mm from each other, sequential tying of the two ligatures and cutting the fistula between them.
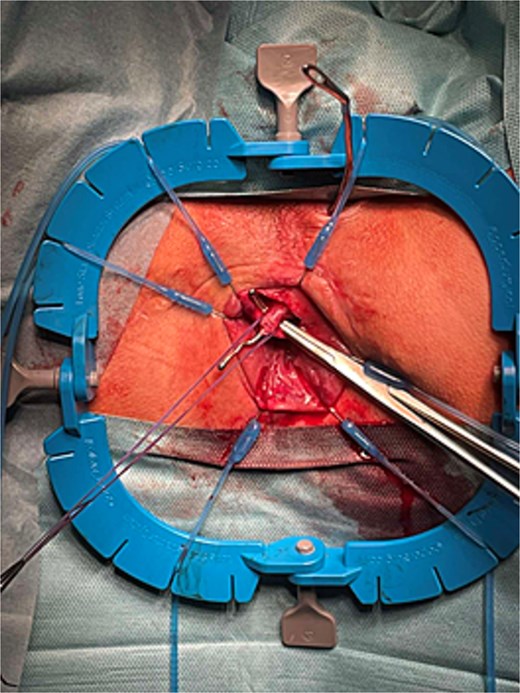
Dissected intersphincter segment of the main fistula tract and first suture ligature placed.
–Closure of the internal opening of the fistula tract with Mucosal Advancement Flap (MAF) (Fig. 7) by excision of the internal opening area, dissection and shaping of a mucosal-submucosal flap, Z-shaped suture of the internal opening in depth at the level of the internal anal sphincter—IAS, distal pulling of the flap and suturing it to the surrounding edges of the defect, also capturing fibers from the IAS distally.

Formed mucosal flap covering the internal opening of the fistula.
The early postoperative period was uneventful, on the 5th postop day when she was discharged. The patient was administered nonsteroidal anti-inflammatory drugs for 5 days and mild laxatives for about 14 days with an appropriate dietary regimen. The follow-up period is 11 months (Fig. 8) and continues to the present, with the patient reporting no incontinence symptoms—neither for gas nor for feces, and she has preserved muscle tone of the anal sphincter complex—rest and squeeze tone.

View of the operative field at the 11th postoperative month.
Discussion
The combination of different techniques is a phenomenon [13] and represents an expression of the aspiration of many surgeons to combine different operative modalities as hybrid techniques in the treatment of perianal fistulas in order to improve the results [14, 15]. There is also a somewhat unintentional desire to present ever-better results at the beginning of the introduction of a new, potentially promising technique into practice. Other authors describe combining the trans anal flap repair (TAFR) technique with the addition of a fibrin matrix plug in the fistula tract, with the results again showing unsatisfactory variations of 25%–70% success rate [16, 17], in contrast to the use of the plug technique alone [18–20]. Another study by Wilhelm et al. [21] described the use of laser-assisted fistula treatment (LAFT) combining it with MAF and achieving fistula eradication in only 67%, a result identical to that of using the LAFT technique alone [22]. Other authors from the Netherlands–van Onkelen et al. [23] reported disturbingly unsatisfactory results with such a combination - a success rate of only 51% of cases [24]. However, our single-center opinion is that there is some theoretical basis for combining the pure flap technique with additional methods—mechanical debridement of the fistula tract + LIFT in a high transsphincteric or other type of complex fistula, with a morphology suitable for combining these techniques [25].
In 10 of our cases we combined LIFT with PTAF technique and follow-up from 11 to 24 months showed only 2 cases of recurrence as transsphincteric, the recurrent fistula appeared as intersphincteric.
In specific clinical cases of complex perianal fistulas with more than one risk factor for disease recurrence—degree of ‘complexity’ of the fistula, obesity, smoking, diabetes, compromised immunity, etc., as well as the original goal of preserving the continence of the anal sphincter complex, the combination of two or more sphincter-preserving techniques is a good prerequisite for minimizing the risk of recurrence. Further prospective randomized clinical trials are needed to extract sufficiently stable data on the feasibility of such a clinical surgical approach.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}