





Abstract
A 75-year-old man presented to our hospital with fever and bloody sputum. Chest computed tomography revealed a mass lesion occupying the left lower lobe with surrounding infiltrative shadows. 18F-fluoro-2-deoxy-glucose positron emission tomography demonstrated high 18F-fluoro-2-deoxy-glucose uptake in the pulmonary mass, left hilar lymph nodes, and right mediastinal lymph node. Transbronchial biopsy confirmed squamous cell carcinoma. The patient was diagnosed with clinical stage IIIC non-small cell lung cancer, and chemoradiotherapy was planned. However, 21 days after the biopsy, he developed acute empyema. Decortication was successfully performed by video-assisted thoracic surgery. Postoperatively, the antimicrobial agent was switched from meropenem hydrate to linezolid after methicillin-resistant Staphylococcus aureus was detected in the pleural effusion culture. The chest tubes were removed 7 days after surgery, and the patient was discharged 1 month after surgery. Chest computed tomography at 1.5 months postoperatively showed no recurrence of empyema, and chemotherapy for advanced non-small cell lung cancer was initiated.
Introduction
Respiratory tract infection after bronchoscopy has been reported to occur in 1.4%–6.3% of cases [1–5]. Lung abscess or empyema following bronchoscopy in patients with lung cancer is much rarer, with an incidence of ~0.3% [5, 6]. In recent years, the incidence of post-bronchoscopic lung abscesses in patients with lung cancer has reportedly increased with the advancement of bronchoscopic techniques, such as endobronchial ultrasound-guided transbronchial biopsy with a guide sheath [5].
Surgical intervention has been reported to effectively control acute empyema in patients with advanced lung cancer, allowing for subsequent chemotherapy or pulmonary resection once the infection is managed [6–8]. By contrast, the prognosis of acute empyema in patients with pleural dissemination of lung cancer has been described as very poor [6], and the prognosis for those with unresectable lung cancer remains unclear.
Methicillin-resistant Staphylococcus aureus (MRSA) is the most common cause of infections due to multidrug-resistant bacteria and has been associated with high mortality rates. For example, the in-hospital mortality of pulmonary infections caused by S. aureus bacteremia (SAB) was reported to range from 41.6% to 62.0% up until the past decade [9, 10]. However, a moderate and progressive decline in SAB-related mortality has been noted over recent decades, although MRSA bacteremia still carries a significantly higher mortality rate than methicillin-sensitive S. aureus bacteremia, even in the current era [11].
We herein report the successful treatment of a patient with inoperable non-small cell lung cancer (NSCLC) who developed MRSA empyema after bronchoscopy and subsequently underwent decortication.
Case report
A 75-year-old man who had undergone right upper lobectomy for NSCLC 7 years earlier presented to our hospital with fever and bloody sputum. His medical history included chemoradiation therapy followed by surgery for hypopharyngeal cancer and a 40-pack-year smoking history.
Chest computed tomography (CT) revealed a mass lesion occupying the left lower lobe of the lung with surrounding infiltrative shadows (Fig. 1a and b). 18F-fluoro-2-deoxy-glucose (FDG) positron emission tomography demonstrated high FDG uptake in the pulmonary mass, left hilar lymph nodes, and right mediastinal lymph node (Fig. 1c–e). Bronchoscopy revealed obstruction of the bronchus of the left lower lobe (Fig. 1f), and transbronchial biopsy confirmed a diagnosis of squamous cell carcinoma. The patient was diagnosed with clinical stage IIIC NSCLC, and chemoradiotherapy was planned. However, 21 days after the transbronchial biopsy, he returned with a fever. Laboratory tests showed elevated white blood cell count (18 560/μl) and C-reactive protein level (23.34 mg/dl). Chest CT demonstrated an increased left pleural effusion (Fig. 2a and b).
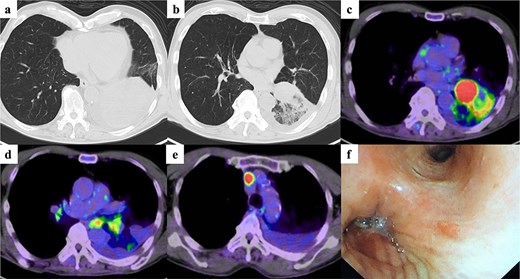
Imaging and bronchoscopic findings before diagnosis. Chest computed tomography showing (a) a mass lesion and (b) an infiltrative shadow in the left lower lobe of the lung. 18F-fluoro-2-deoxy-glucose (FDG) positron emission tomography demonstrating high FDG uptake in (c) the pulmonary lesion, (d) the left hilar lymph node, and (e) the right mediastinal lymph node. (f) Bronchoscopy revealing obstruction of the bronchus of the left lower lobe.
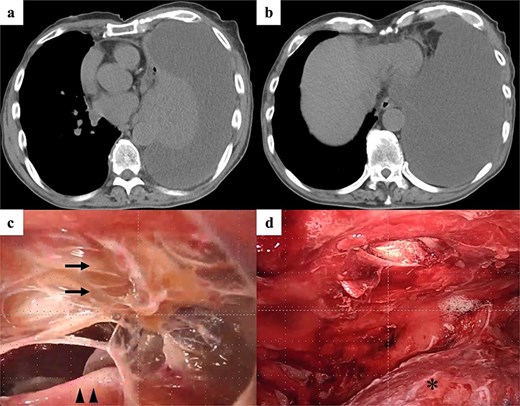
Intraoperative findings and surgical procedure. (a and b) Chest computed tomography showing an increase in the left pleural effusion. (c) Intraoperative findings showing fibrin precipitation (arrows) around the left lung (arrowheads). (d) Decortication around the left lung (asterisk) successfully performed by video-assisted thoracic surgery.
The patient was admitted on an emergency basis, and thoracic drainage was performed. The pleural effusion had a pH of 7.120, and clusters of Gram-positive cocci were observed on Gram staining. Despite continuous chest drainage, surgery was required because of residual pleural fluid in multiple locations within the left thoracic cavity. Massive pleural effusion and fibrin deposits were observed intraoperatively (Fig. 2c), and successful decortication was performed via video-assisted thoracic surgery (Fig. 2d).
Postoperatively, the antimicrobial agent was switched from meropenem hydrate to linezolid after MRSA was detected in the pleural fluid culture. The patient’s white blood cell count and C-reactive protein level decreased rapidly, and the chest tubes were removed 7 days after surgery. The anti-MRSA agent was temporarily changed to vancomycin because of thrombocytopenia, and the antibiotic therapy was discontinued prior to discharge, which occurred 1 month after surgery (Fig. 3).
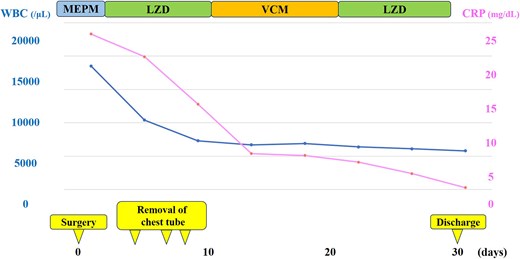
Clinical course after surgery. Postoperatively, the antimicrobial agent was switched from MEPM to LZD after methicillin-resistant Staphylococcus aureus was detected in the pleural effusion culture. The WBC count and CRP level decreased rapidly, and the chest tubes were removed by postoperative day 7. The anti–methicillin-resistant S. aureus agent was temporarily changed to VCM because of thrombocytopenia, then discontinued, and the patient was discharged 1 month after surgery. MEPM, meropenem hydrate; LZD, linezolid; VCM, vancomycin; WBC, white blood cell; CRP, C-reactive protein.
Chest CT performed 1.5 months after surgery showed no recurrence of empyema (Fig. 4a and b). The patient subsequently received daily low-dose carboplatin (30 mg/m2) with concurrent thoracic radiotherapy (60 Gy), followed by maintenance therapy with durvalumab (1500 mg/body, every 4 weeks). No recurrence of empyema was observed, and reduction of the left lower lobe lesion was confirmed 4 months after surgery (Fig. 4c and d).
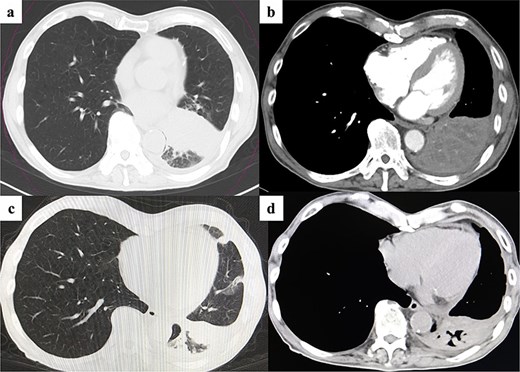
Postoperative imaging and treatment outcome. (a and b) Chest computed tomography showing no recurrence of empyema 1.5 months after surgery. (c and d) At 4 months after surgery, chest CT demonstrating no recurrence of empyema and reduction of the left lower lobe lesion following chemoradiotherapy and subsequent maintenance therapy with an immune checkpoint inhibitor.
Discussion
In the present report, we have described a patient with inoperable NSCLC who developed MRSA empyema after bronchoscopy and was successfully treated with decortication. Although post-bronchoscopy empyema remains rare, patients who develop it may need to delay or cancel their planned cancer therapy [5]. Furthermore, the prognosis of acute empyema in patients with pleural dissemination of lung cancer is reportedly very poor. By contrast, surgical intervention has been shown to effectively control acute empyema in patients with advanced lung cancer, allowing for subsequent chemotherapy or pulmonary resection once the infection is managed [6, 7]. Although infection control was achieved in nearly 90% of patients who had empyema with carcinomatous pleuritis due to lung cancer through thoracoscopic surgery, only 25% of these patients were able to initiate chemotherapy [6]. Conversely, ~90% of patients who had empyema with lung cancer but without carcinomatous pleuritis were able to receive chemotherapy or undergo surgery for lung cancer after infection control [8]. These findings highlight the importance of prompt infection management because patients who have advanced lung cancer without carcinomatous pleuritis may still be eligible for subsequent cancer treatment once the infection is controlled, as demonstrated in the present case.
MRSA is the most common cause of infections due to multidrug-resistant bacteria and has long been associated with high mortality rates [9, 10]. For example, the in-hospital mortality rate among patients with MRSA pneumonia was reported to be ~30% during the past decade [12–14]. Although a moderate and progressive decline in mortality due to SAB has been observed over the past decades, MRSA bacteremia still carries a significantly higher mortality rate than methicillin-sensitive S. aureus bacteremia, even in the current era [11]. However, the prognosis and optimal treatment for MRSA empyema remain unclear because only a few cases have been reported [15]. Therefore, further studies are needed to clarify the prognosis and establish appropriate treatment strategies for MRSA empyema in the future.
In conclusion, we have reported a case involving a patient with inoperable NSCLC who developed MRSA empyema after bronchoscopy and was successfully treated with decortication. Prompt infection control is crucial because patients with advanced lung cancer may still be able to receive further cancer treatment once the infection is adequately managed.
Acknowledgements
We thank Angela Morben, DVM, ELS, from Edanz (https://jp.edanz.com/ac), for editing a draft of this manuscript.
Author contributions
N.M., M.I., and S.I. performed the surgery. N.M. acquired the data and drafted the manuscript. All other authors contributed to data collection, and they critically reviewed the manuscript. All authors approved the final version of the manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Conflicts of interest
The authors declare that they have no competing interests.
Funding
This work was supported by Grants-in-Aid for Scientific Research of Japan Society for the Promotion of Science (grant no.: 23K08326).
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics approval and consent to participate
This work does not require ethical considerations or approval. Informed consent to participate in this study was obtained from the patient.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}