





Abstract
Peptic ulcer perforation (PUP) is a life-threatening surgical emergency. Persistent perforation after conventional repair is rare, and minimally invasive salvage techniques are infrequently reported. We present a case where endoscopic pigtail catheter drainage offered a novel solution for a persistent leak. A 33-year-old man with substance use history developed generalized peritonitis after an intentional drug overdose. Emergency laparotomy revealed a 7 × 7 mm prepyloric perforation, repaired with a Graham patch. Premature oral intake led to a larger persistent perforation 5 days later, requiring repeat surgical repair. Persistent leakage continued for nearly a month and was successfully managed using an endoscopically placed pigtail catheter without a stent. The patient recovered completely, as confirmed at a 6-week follow-up. Endoscopic pigtail catheter placement is a minimally invasive, organ-preserving salvage therapy for persistent PUP after failed surgical repair. Further studies are needed to establish standardized protocols.
Introduction
Perforated peptic ulcer (PUP) remains a significant cause of the acute abdomen, carrying appreciable morbidity and mortality [1, 2]. The standard operative approach for small-to-moderate perforations has traditionally been primary closure with an omental patch (Graham patch), owing to its technical simplicity and organ-preserving nature. [3–5] However, recent evidence suggests that the superiority of omental patch reinforcement over primary closure alone remains controversial, with some studies demonstrating no significant difference in outcomes [6, 7]. However, postoperative failure of primary repair, manifesting as a persistent leak or recurrent perforation, is a feared complication. It is strongly associated with increased morbidity, prolonged hospitalization, and higher mortality [2, 6, 8]. Key predictors of repair failure include delayed presentation, large perforation size, friable tissue margins, septic physiology, and factors like substance use that impair healing [5, 6, 8, 9].
When primary repair fails, therapeutic options range from conservative management to re-laparotomy. Recently, endoscopic strategies have expanded. While covered stents, over-the-scope clips, and endoscopic vacuum therapy (EndoVAC) are options, each has limitations [10, 11]. Endoscopic internal drainage (EID) using double-pigtail catheters is a low-cost method to drain perigastric collections and promote healing by creating an internal controlled drainage route [2, 12]. Despite this growing armamentarium, the role of endoscopic pigtail drainage specifically for persistent PUP after failed omental patch repair is not well defined. This report presents a patient with a persistent prepyloric perforation after two consecutive Graham patch repairs, whose persistent leakage was successfully controlled with this technique.
Case presentation
A 33-year-old Persian man with a history of chronic alcohol, opium, and non-steroidal anti-inflammatory drugs (NSAID) use presented to the emergency department with acute severe epigastric pain. He had intentionally ingested 20 diazepam tablets. On examination, he was febrile (38.5°C), tachycardic, and hypotensive, with signs of generalized peritonitis.
Initial labs revealed leukocytosis (white blood cell 18 200/μl), elevated C-reactive protein (182 mg/l), and acute kidney injury (creatinine 1.9 mg/dl), suggesting sepsis. An erect chest X-ray demonstrated free subdiaphragmatic air (Fig. 1).
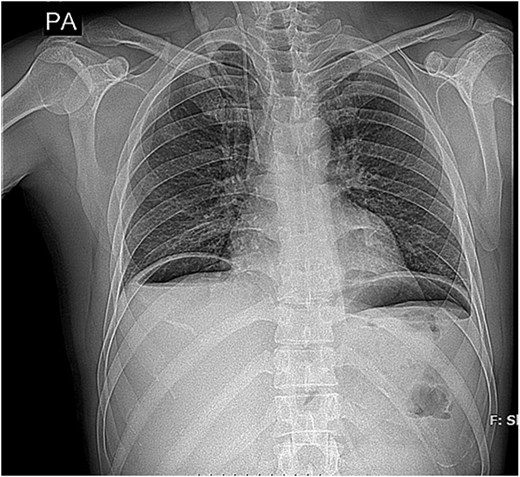
Upright chest radiograph showing free subdiaphragmatic air beneath the right hemidiaphragm (arrows), consistent with hollow viscus perforation.
The patient underwent emergency laparotomy, which revealed a 7 × 7 mm prepyloric perforation with gross peritoneal contamination. A Graham omental patch repair was performed. Postoperatively, he was admitted to the intensive care unit (ICU). Despite initial improvement, he developed persistent sepsis and bilious drain output on Day 5. An intra-abdominal drain had been placed adjacent to the repair site during surgery. Persistent bilious output from the drain raised suspicion for ongoing leakage. A computed tomography (CT) scan showed extraluminal contrast leakage, confirming a persistent perforation (Fig. 2). On Day 6, he underwent a repeat laparotomy. A larger 1 × 1.5 cm perforation was identified and closed with another Graham patch. However, bilious drainage persisted.

Contrast-enhanced CT scan showing extraluminal contrast leakage and localized fluid collection adjacent to the anterior gastric wall, indicating postoperative leak at the previous repair site.
The leak remained localized without evidence of diffuse peritonitis, making it suitable for minimally invasive internal drainage approach. On postoperative Day 14, an endoscopic approach was pursued. Endoscopy confirmed a persistent leak at the prior repair site. A double-pigtail catheter was placed transgastrically, bridging the leak to provide internal drainage into the stomach (Fig. 3). This hybrid approach led to rapid clinical improvement. Within 72 h, sepsis markers normalized, and drain output diminished. The patient was gradually advanced to an oral diet and discharged on postoperative Day 32. At the 3-month follow-up, he remained asymptomatic with no recurrence. His total ICU stay was 17 days (Fig. 4) (Table 1).

Endoscopic image showing transgastric placement of a double-pigtail catheter across the leak site for internal drainage.
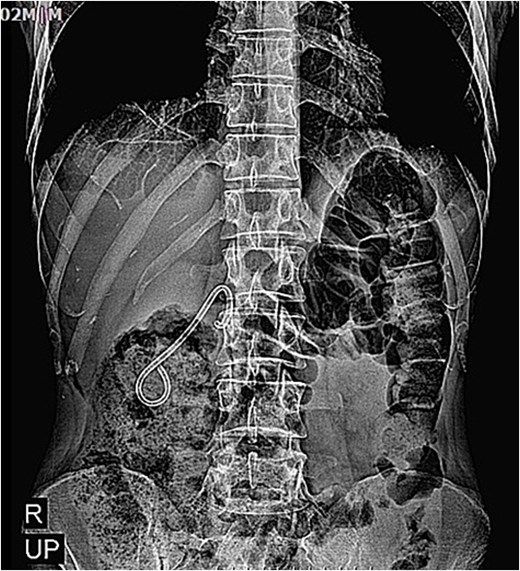
Upright abdominal radiograph at 3-month follow-up (2 June 2025) showing complete resolution of previous fluid collections and absence of free air.
Clinical timeline
| Date | Hospital day | Event/clinical action | Details |
|---|---|---|---|
| 13 March 2025 | Day 0 | Intentional ingestion of 20 diazepam tablets (100 mg) | Patient with chronic alcohol and opium use |
| 13 March 2025 | Day 0 | Emergency laparotomy | 7 × 7 mm prepyloric perforation repaired with Graham omental patch; transferred to ICU postoperatively |
| 13–16 March 2025 | Days 0–3 | ICU care | Postoperative monitoring and supportive care |
| 16 March 2025 | Day 3 | Transfer to the surgical ward | Stable, continued recovery |
| 18 March 2025 | Day 5 | Recurrent abdominal pain and sepsis | After premature oral intake, re-exploration indicated |
| 18 March 2025 | Day 5 | Re-laparotomy | 1 × 1.5 cm anterior gastric perforation repaired again with Graham patch; ICU care postoperatively |
| 18 March–13 April 2025 | Days 5–31 | ICU + ward care | Persistent leak managed conservatively; patient stabilized for endoscopic intervention |
| 13 April 2025 | Day 31 | Endoscopic pigtail drainage | No stent inserted; leak successfully controlled; avoided third laparotomy |
| 13 April–24 April 2025 | Days 31–42 | Ward care | Stable recovery and discharge planning |
| 2 June 2025 | Follow-up | Outpatient evaluation | Complete recovery without recurrence |
Discussion
Primary closure with or without omental patch reinforcement remains widely practiced for PUP; however, the added benefit of the Graham patch over simple closure remains debated in the literature [6, 7]. However, postoperative leaks can occur, especially in patients with friable tissue or non-adherence to dietary restrictions. Early oral intake and non-adherence to postoperative dietary restrictions have been associated with increased risk of repair failure and leakage in gastrointestinal perforations [13]. In this case, the persistent perforation was likely exacerbated by premature oral intake and comorbidities like chronic substance use, emphasizing the need for strict postoperative monitoring.
When primary repair fails, minimally invasive endoscopic techniques are increasingly valuable salvage therapies [7]. Covered self-expanding metal stents can exclude a leak but risk migration and tissue overgrowth. Endoscopic clipping and EndoVAC are alternatives for smaller defects. EID with double-pigtail stents offers a hybrid approach, allowing for internal drainage of perigastric collections while avoiding repeat laparotomy. Widely reported for bariatric surgery leaks, its use in refractory PUP is a logical extension [14].
In cases of failed primary repair, several surgical alternatives have been described, including jejunal serosal patch (jejunal onlay), antrectomy with reconstruction, or wedge resection of the perforation site. These approaches are typically reserved for large defects, non-viable tissue, or repeated repair failure but are associated with increased operative morbidity and physiological stress, particularly in critically ill patients.
In our patient, this approach successfully controlled the leak, facilitated recovery, and preserved gastric anatomy. The decision to use EID was guided by the patient’s hemodynamic stability and the favorable perforation characteristics.
Management of complicated PUP is resource-intensive, often requiring prolonged ICU stays [13]. This patient’s 17-day ICU course reflects the significant morbidity associated with this condition. Practical insights from this case include the value of endoscopic pigtail drainage as a salvage strategy, the necessity of careful radiologic and endoscopic assessment, and the importance of multidisciplinary collaboration.
Given the rarity of refractory PUP, large randomized trials are unlikely to be feasible. Future evidence may be better generated through multicenter registries, pooled case series, and collaborative prospective observational studies comparing endoscopic and surgical salvage strategies.
Limitations of this report include its single-case design. Future studies should focus on defining the indications, timing, and comparative efficacy of pigtail drainage versus other modalities for refractory PUP.
Conclusion
Persistent peptic ulcer perforation is a life-threatening emergency with significant morbidity. While the Graham patch is the standard initial approach, postoperative leakage can occur. This case illustrates that EID using a double-pigtail stent can serve as a safe, minimally invasive, organ-preserving salvage therapy after failed surgical repairs, even in complex patients. This hybrid approach successfully controlled persistent leakage, avoided a third laparotomy, and facilitated complete healing. With careful patient selection and multidisciplinary coordination, it is an effective alternative to major reoperation. Future prospective studies are warranted to establish standardized protocols for its use in this context.
Acknowledgements
The authors would like to express their gratitude to the authorities of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran, for their technical and editorial assistance. The authors also express their profound appreciation to Mr. Masoud Dodangeh for his insightful guidance, constructive recommendations, and dedicated contribution to the refinement and improvement of this manuscript.
Author contributions
Milad Dodangeh (Conceptualization, Patient Management, Performed the surgery, Writing—original draft, Writing—review & editing), Hamidreza Kanani (Conceptualization, Patient Management, Performed the surgery), and Mohsen Soori (Patient Management, Writing—review & editing, Supervision). All authors have read and approved the final manuscript and guarantee the accuracy of the manuscript. All members of this research team reviewed the manuscript and data and assume full responsibility for the content.
Conflicts of interest
There were no conflicts of interest among all authors.
Funding
This study received no funding.
Data availability
The datasets used during this study will be available from the corresponding author upon reasonable request.
Ethical approval
This case report does not require ethical approval from our institution as it involves a single patient case that is anonymized and does not include any identifiable personal information.
Consent to publish
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Guarantor
Mohsen Soori.
Patient perspective
When I was admitted after taking an overdose of sleeping pills, I did not realize the seriousness of my condition. The first surgery relieved my pain, but the complication came back, and I became afraid of another major operation. I was very weak and hopeless. After the doctors explained a new minimally invasive method, the endoscopic drainage, I agreed to it. I am thankful that this procedure worked and avoided another surgery. Now, months later, I feel healthy and grateful for the care I received.

{kind=link}
{kind=link}
{kind=link}
{kind=link}