





Abstract
Migration of plastic biliary stents is a recognized complication of endoscopic retrograde cholangiopancreatography (ERCP), although it is usually asymptomatic and self-limiting. Intestinal perforation due to stent migration is rare, and involvement of Meckel’s diverticulum is exceedingly uncommon. We report a 70-year-old woman who presented with acute abdomen approximately one year after ERCP with placement of a 10F–10 cm plastic biliary stent for choledocholithiasis. Computed tomography revealed small bowel obstruction and a linear hyperdense intraluminal structure consistent with a foreign body. Emergency surgery identified a migrated biliary stent impacted within a Meckel’s diverticulum located 40 cm proximal to the ileocecal valve. One end of the stent was lodged in the diverticulum, while the opposite end perforated the adjacent ileal loop, resulting in localized peritonitis. Segmental small bowel resection with primary side-to-side anastomosis was performed. The postoperative course was complicated by respiratory failure requiring prolonged ventilatory support; however, the patient recovered and was discharged in good condition. This case highlights a rare bidirectional perforation mechanism caused by long-term indwelling plastic biliary stent migration. In patients with a history of ERCP presenting with acute abdomen, migrated stents should be considered in the differential diagnosis. Regular surveillance and timely removal of plastic biliary stents are essential to prevent severe late complications.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is a widely used and effective therapeutic modality for the management of biliary tract diseases. Plastic biliary stents are frequently preferred, particularly in cases of choledocholithiasis and benign biliary obstruction; however, stent-related complications are not entirely negligible. Distal migration occurs in ~5%–10% of plastic biliary stents and, in most cases, the stent passes through the gastrointestinal tract without causing clinical symptoms [1, 2]. Nevertheless, in rare circumstances, a migrated stent may become impacted within the intestine, leading to serious complications such as obstruction, inflammation, or perforation [3, 4].
Meckel’s diverticulum is the most common congenital anomaly of the gastrointestinal tract and remains asymptomatic in the majority of individuals [5]. However, impaction of foreign bodies within the diverticulum may result in complications including diverticulitis, ulceration, and perforation [6, 7]. Although cases of migrated foreign bodies causing perforation of Meckel’s diverticulum have been reported in the literature, to the best of our knowledge, no case has been described in which migration into the diverticulum resulted in perforation of the adjacent ileal loop. Such a condition may be associated with a potentially high risk of morbidity.
In this article, we present a case of acute abdomen caused by a biliary stent that migrated and became lodged within a Meckel’s diverticulum, leading to ileal perforation in a patient who had undergone ERCP for choledocholithiasis approximately one and a half years earlier.
Case presentation
A 70-year-old female patient with a history of type 2 diabetes mellitus, hypertension, chronic atrial fibrillation, and chronic obstructive pulmonary disease (COPD) presented to the emergency department with progressively worsening abdominal pain. She had undergone ERCP for choledocholithiasis one year earlier, during which a 10F–10 cm plastic biliary stent was placed following balloon extraction.
She presented with diffuse abdominal pain, distension, and nausea. Physical examination revealed signs of peritoneal irritation. Upright abdominal radiography and abdominal computed tomography (CT) demonstrated multiple air–fluid levels in the small bowel loops and a linear hyperdense structure within the intestinal lumen consistent with a foreign body (Fig. 1). These findings suggested acute abdomen secondary to mechanical small bowel obstruction.
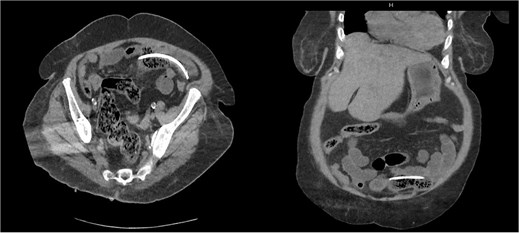
Abdominal computed tomography demonstrating a linear hyperdense intraluminal structure consistent with a migrated biliary stent.
Emergency laparoscopic exploration was planned; however, due to dense purulent fluid and extensive intra-abdominal adhesions, the procedure was converted to open surgery. Systematic evaluation of the small intestine revealed a Meckel’s diverticulum ~40 cm proximal to the ileocecal valve containing a rigid foreign body. Its distal end had perforated the adjacent ileal segment. The object was identified as a migrated biliary stent (Fig. 2).
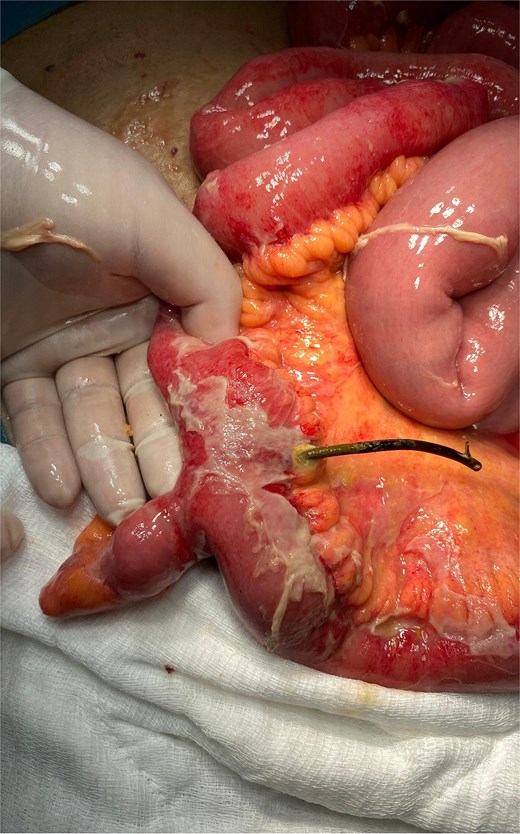
Intraoperative view showing a migrated plastic biliary stent impacted within a Meckel’s diverticulum, with perforation of the adjacent ileal segment.
A segmental resection of ~20 cm of small intestine, including the diverticulum and perforation site, was performed, followed by side-to-side stapled anastomosis. After irrigation and drainage, the operation was completed, and the patient was transferred intubated to the intensive care unit.
Postoperatively, prolonged ventilatory support was required due to COPD-related respiratory failure. She was managed with mechanical ventilation, high-flow nasal oxygen therapy, and intermittent noninvasive ventilation. Episodes of hypernatremia, hypercalcemia, and atrial fibrillation were treated medically. From postoperative day 13 onward, respiratory and neurological status improved, and she was successfully extubated. She tolerated oral intake and was discharged on postoperative day 40 after an uneventful recovery.
Discussion
Although biliary stent migration is usually asymptomatic, severe complications such as intestinal perforation are exceedingly rare. Due to their structural characteristics, plastic biliary stents are known to migrate more frequently than metal stents [2, 8]. Following migration, impaction of the stent within the intestine is more likely in the presence of anatomical narrowings, inflammatory changes, or diverticular disease [3, 9].
Meckel’s diverticulum represents a high-risk location for foreign body impaction. Intraluminal stasis and the narrow neck of the diverticulum may facilitate retention of foreign bodies, predisposing to local inflammation and perforation [5, 6]. Various foreign bodies causing perforation after impaction within a Meckel’s diverticulum have been reported in the literature; however, cases in which a migrated biliary stent lodges within the diverticulum and subsequently perforates the adjacent ileal loop are exceedingly rare. In the case reported by Topal et al. [10], a migrated biliary stent was shown to perforate the Meckel’s diverticulum itself. In contrast, in our case, impaction of one end of the stent within the Meckel’s diverticulum mechanically prevented further distal migration, while the opposite end perforated the adjacent ileal segment. This bidirectional mechanism not only increases the rarity of the case but also appears to contribute to a more severe clinical presentation.
CT is the preferred imaging modality in suspected foreign body–related perforations due to its high sensitivity and specificity in demonstrating both direct and indirect signs of bowel perforation [11]. Once perforation occurs, urgent surgical intervention is mandatory. Appropriate surgical management includes diverticulectomy or segmental small bowel resection with primary anastomosis, depending on the extent of involvement.
This case also highlights the importance of regular follow-up and timely removal of plastic biliary stents. International guidelines recommend that plastic biliary stents be removed or exchanged ideally within three months [8]. Inadequate follow-up of indwelling stents may result in late complications such as migration, obstruction, and, rarely, life-threatening perforation.
Conclusion
Although rare, migrated biliary stents impacted within the intestine can lead to life-threatening complications. This case presents an unusual clinical scenario in which a long-term indwelling plastic biliary stent became lodged within a Meckel’s diverticulum, resulting in diverticulitis and ileal perforation. In patients with a history of ERCP presenting with acute abdomen, stent migration should always be considered in the differential diagnosis. Early recognition and timely surgical intervention are crucial for reducing morbidity. Regular surveillance and appropriate removal of plastic biliary stents remain essential to prevent such complications.
Conflicts of interest
None declared.
Funding
None declared.
Consent
Written informed consent was obtained from the patient.

{kind=link}
{kind=link}