





Abstract
Spigelian hernia is a rare ventral abdominal wall hernia occurring through a defect in the Spigelian aponeurosis along the semilunar line, accounting for 1%–2% of all abdominal wall hernias, with a high risk of incarceration due to its narrow and rigid fascial neck. A sacless variant, in which only preperitoneal fat protrudes without a peritoneal sac, is exceptionally rare and poses a diagnostic challenge. A 52-year-old male presented with a reducible left lower abdominal swelling and intermittent pain. Diagnostic laparoscopy showed intact peritoneum with no visible hernia defect. A strong clinical suspicion precluded conversion to open exploration, revealing a 2 × 3 cm defect in the Spigelian aponeurosis containing preperitoneal lipomatous tissue without a peritoneal sac. A preperitoneal mesh repair was undertaken. Sacless Spigelian hernia being extremely rare, a high index of suspicion and readiness for open exploration are essential when imaging and laparoscopy are inconclusive.
Introduction
Spigelian hernia is a rare ventral abdominal wall hernia occurring through a defect in the Spigelian aponeurosis between the lateral border of the rectus abdominis muscle and the semilunar line. It accounts for ~1%–2% of all abdominal wall hernias and is frequently underdiagnosed due to its interparietal location and intact external oblique aponeurosis [1, 2].
The semilunar line was first described by Adriaan van der Spiegel in 1645, and the hernia itself was later defined by Klinkosch in 1764 [1, 3]. Spigelian hernia most commonly occurs within a transverse zone ~6 cm above the interspinous plane, known as the ‘Spigelian belt,’ where the abdominal wall is structurally weakest [1, 4].
A characteristic feature of Spigelian hernia is its narrow and rigid fascial neck, which confers a high risk of incarceration and strangulation, reported in up to 30% of cases [1, 5]. Consequently, elective surgical repair is recommended even in asymptomatic patients.
A sacless Spigelian hernia, in which only preperitoneal fat protrudes through the aponeurotic defect without formation of a peritoneal sac, represents an exceptionally rare variant and poses a significant diagnostic and intraoperative challenge. We report such a case and discuss its diagnostic dilemma and surgical management.
Case report
A 52-year-old male, a known diabetic and hypertensive, presented with a bulge over the left lower abdomen for 5 months associated with intermittent abdominal pain for 2 months. The swelling increased on straining and disappeared on lying down. There was no history of trauma or previous abdominal surgery.
On clinical examination, a reducible swelling was noted in the left lower abdomen with a positive cough impulse. The fascial defect was not clearly appreciable (Fig. 1A).
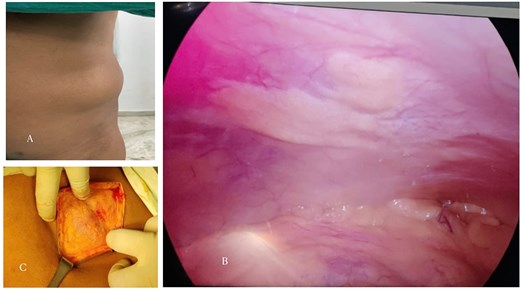
(A) Preoperative clinical photograph showing a reducible swelling over the left lower abdominal wall along the semilunar line (Spigelian belt region). (B) Laparoscopic view demonstrating intact peritoneum without visible hernia sac or defect. (C) Open intraoperative image revealing a 2 × 3 cm defect in the left Spigelian aponeurosis containing preperitoneal lipomatous tissue without a peritoneal sac, consistent with a sacless Spigelian hernia.
Ultrasonography of the abdomen revealed only small renal calculi. A computed tomography scan of the abdomen (CT KUB) did not demonstrate any abdominal wall defect. The CT images were reviewed with a radiologist; however, no definitive hernia could be identified.
In view of persistent clinical suspicion, diagnostic laparoscopy was planned. Pneumoperitoneum was created using an open supra-umbilical technique. A 10-mm camera port was placed infra-umbilically, and a 5-mm working port in the midline between the umbilicus and pubic symphysis.
Laparoscopic examination revealed an intact peritoneal lining with no visible hernia sac or abdominal wall defect, even after pneumoperitoneum (Fig. 1B).
Given the strong clinical suspicion, the procedure was converted to open surgery. A left transverse incision was made over the swelling. On exploration, a 2 × 3 cm defect was identified in the Spigelian aponeurosis containing preperitoneal lipomatous tissue without a peritoneal sac, consistent with a sacless Spigelian hernia (Fig. 1C).
A preperitoneal (sublay) space was created by blunt dissection, and a 10 × 15 cm polypropylene mesh was placed and fixed at four corners (Fig. 2A and B).

(A, B) Placement of polypropylene mesh in the preperitoneal (sublay) plane adequately covering the defect.
The postoperative course was uneventful. The patient tolerated oral intake from postoperative day 1 and ambulated without difficulty. There were no wound-related complications or seroma formation. He was discharged on postoperative day 7 in stable condition. On follow-up at 2 weeks, the wound had healed well with no residual swelling. The patient has been followed up for 1 year postoperatively, during which he has remained asymptomatic with no evidence of recurrence or residual bulge on clinical examination.
Discussion
Spigelian hernia is an uncommon ventral hernia occurring through a defect in the Spigelian aponeurosis between the lateral border of the rectus abdominis muscle and the semilunar line. It most commonly develops within the Spigelian belt, a transverse zone ~6 cm above the interspinous plane [1, 4].
The interparietal location of the hernia sac and the presence of an intact external oblique aponeurosis often mask the swelling on physical examination, resulting in delayed or missed diagnosis [2, 6].
Most patients present with localized abdominal pain, with or without a palpable swelling. Approximately two-thirds of patients present with abdominal pain or discomfort without a palpable lump [7].
Spigelian hernia typically affects elderly individuals, with a reported median age of 60–65 years and a female predominance [1, 5]. Predisposing factors include obesity, chronic cough, multiparity, and conditions associated with increased intra-abdominal pressure [5, 8].
A defining characteristic of Spigelian hernia is its high risk of incarceration and strangulation, reported to range between 17% and 30% [1, 5, 9]. This is attributed to the narrow and rigid fascial neck, which is often less than 2 cm in diameter [4, 9]. Current European Hernia Society and American Hernia Society guidelines therefore recommend elective surgical repair of all diagnosed Spigelian hernias, even in asymptomatic patients [10].
Clinical diagnosis is challenging due to the deep location of the hernia. Ultrasonography is recommended as the first-line imaging modality, particularly in thin patients, while contrast-enhanced CT scan is considered the gold standard in equivocal cases [6, 7, 11]. However, sacless variants of Spigelian hernia represent a unique diagnostic dilemma. In such cases, only preperitoneal fat herniates through the aponeurotic defect without formation of a peritoneal sac, resulting in normal-appearing peritoneum on imaging and laparoscopy, as in the present case.
Surgical repair is the definitive treatment. Both open and minimally invasive approaches are validated. Laparoscopic repair offers advantages such as reduced postoperative pain, shorter hospital stay, and lower wound morbidity [11, 12]. Several laparoscopic techniques have been described, including intraperitoneal onlay mesh, transabdominal preperitoneal, and totally extraperitoneal repairs [7, 12–14]. Moreno-Egea et al. reported favorable outcomes with laparoscopic repair compared with open techniques in a prospective randomized trial [15].
Despite the advantages of laparoscopy, open surgery remains important in occult or sacless hernias where laparoscopic visualization may be misleading. In such cases, open exploration remains the most reliable method for identifying the aponeurotic defect and performing definitive repair [2, 6].
Mesh repair is generally recommended due to low recurrence rates. Moreno-Egea et al. demonstrated superior outcomes with mesh repair compared with primary suture repair in a prospective randomized trial [15]. Similar excellent long-term results have been reported by Vos and Scheltinga [9].
In the present case, despite negative imaging and an apparently normal laparoscopic examination, strong clinical suspicion prompted open exploration, leading to identification of a 2 × 3 cm aponeurotic defect containing preperitoneal fat without a peritoneal sac. Sublay mesh repair was performed with an uneventful recovery. At 6-month and 1-year follow-up, the patient remained asymptomatic with no evidence of recurrence.
The present case highlights a rare sacless Spigelian hernia in which preoperative imaging and diagnostic laparoscopy failed to identify the defect due to intact peritoneum. Conversion to open surgery enabled recognition of the aponeurotic defect and successful sublay mesh repair. Hence, underscoring the importance of maintaining a high index of suspicion in such cases for prompt management and early recovery.
Author contributions
All authors contributed to patient management, data collection, manuscript drafting, and approval of the final version.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
None declared.
Ethical approval
Not required for a single case report.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Guarantor
The corresponding author accepts full responsibility for the work.
References
Klinkosch JT. Programma, quo sectiones et demonstrationes suas anatomicas publicas hyemales proponit. In: John JD, editor.

{kind=link}
{kind=link}