





Abstract
Congenital intrinsic obstruction at or near the duodenojejunal junction is exceptionally rare and most commonly results from incomplete embryonic recanalization, leading to the formation of a mucosal web. We report a 7-day-old term male neonate (birth weight 3350 g) who presented with persistent feeding intolerance and intermittent bilious vomiting since birth. Abdominal radiography showed marked dilation of the stomach and duodenum with distal bowel gas. An upper gastrointestinal contrast study revealed a conical narrowing at the duodenojejunal junction. Surgical exploration revealed a mucosal web located immediately distal to the duodenojejunal junction. Given the marked luminal disparity, simple web excision was deemed inadequate, and segmental resection with primary end-to-end jejunojejunal anastomosis was performed. Postoperative recovery was uneventful. Proximal jejunal webs near the duodenojejunal junction are rare but surgically correctable causes of neonatal bilious vomiting and should be considered in the differential diagnosis.
Introduction
Bilious vomiting in neonates constitutes a surgical emergency and requires prompt evaluation. The differential diagnosis includes malrotation with midgut volvulus, Hirschsprung disease, sepsis, and a spectrum of congenital intrinsic or extrinsic intestinal obstructions. Type I atresia, first described by Louw and Barnard [1], is characterized by a mucosal web (also referred to as a mucosal diaphragm) that may result in complete or partial luminal obstruction. Congenital webs most commonly occur in the duodenum, where they typically present with the classic double-bubble sign. In contrast, fenestrated or partially obstructive webs may produce subtle or equivocal radiographic findings. Congenital intrinsic obstruction involving the duodenojejunal junction or proximal jejunum is exceedingly rare [2, 3]. It is also characterized by various clinical presentations. Owing to its atypical location and variable degree of obstruction, diagnosis can be challenging and requires a high index of suspicion combined with careful radiologic and intraoperative assessment. We present a rare case of a congenital mucosal web causing proximal jejunal obstruction located immediately distal to the duodenojejunal junction, highlighting key diagnostic considerations and operative strategies relevant to this unusual anatomical location.
Case report
A 7-day-old term male neonate, delivered vaginally (birth weight 3350 g), presented with persistent feeding intolerance and intermittent bilious vomiting since birth. Prenatal ultrasound was unremarkable, and there was no family history of congenital anomalies. Erect abdominal radiography demonstrated marked dilatation of the stomach and duodenum with preserved distal bowel aeration (Fig. 1A). An upper gastrointestinal contrast study showed significant dilation of the stomach and all four portions of the duodenum, with a sharply tapered, conical narrowing at the duodenojejunal junction (Fig. 1B). The duodenojejunal junction was normally positioned to the left of the spine at the level of the pylorus, with normal passage of contrast into the distal small bowel, thereby excluding intestinal malrotation followed by a tension-free end-to-end jejunojejunal anastomosis (Fig. 2C). Exploratory laparotomy following Kocher’s maneuver revealed a grossly distended stomach and duodenum with pronounced caliber discrepancy at the duodenojejunal junction (Fig. 2A). Normal midgut rotation and fixation were confirmed, with no evidence of volvulus or Ladd’s bands. A mucosal web was identified in the proximal jejunum immediately distal to the duodenojejunal junction (Fig. 2B). Given the substantial luminal disparity, simple longitudinal enterotomy with web excision and transverse closure was avoided. Instead, segmental resection was performed, followed by a tension-free end-to-end jejuno-jejunal (Fig. 2C).
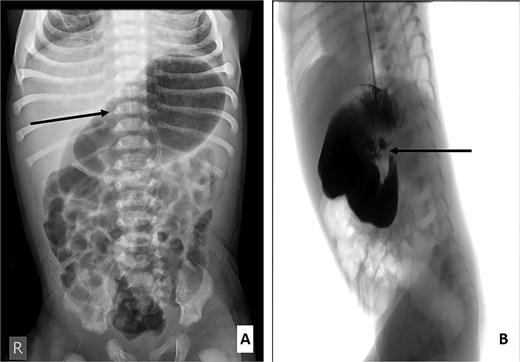
(A) Erect abdominal radiograph showing a markedly distended stomach (arrow) with aeration of the small and large intestines. (B) Contrast study demonstrating a markedly dilated stomach and duodenum with a conical narrowing at the duodenojejunal junction (labeled).
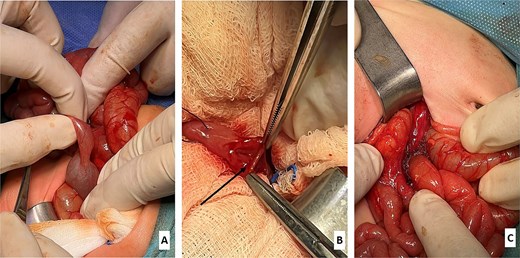
(A) Intraoperative view showing a grossly dilated stomach and duodenum with significant caliber disparity at the duodenojejunal junction. (B) Intraoperative identification of the mucosal web (labeled). (C) Following resection of the mucosal web, an end-to-end jejunojejunal anastomosis was performed distal to the duodenojejunal junction.
The postoperative course was uneventful. Bowel function returned promptly, enteral feeding was gradually initiated and advanced without difficulty, and the patient was discharged on postoperative Day 10. Follow-up at 3 and 6 months showed normal growth and feeding tolerance, with no gastrointestinal symptoms.
Discussion
Intrinsic congenital obstruction of the proximal jejunum immediately distal to the duodenojejunal junction is extremely rare, with only a limited number of cases reported in the literature [2, 4]. These anomalies arise from incomplete embryologic recanalization and manifest as fenestrated or complete mucosal webs. Approximately 8% of all intestinal webs occur in the jejunum [4], and 30%–50% are associated with additional congenital anomalies [4, 5]; none were present in our patient. In the present case, the type I jejunal atresia was localized in the immediate post-duodenojejunal segment. While jejunal webs are uncommon overall, lesions in this proximal location may present either in the neonatal period or later in life with intermittent or nonspecific symptoms. To contextualize our findings, we compiled a focused review of reported pediatric cases of proximal/high type I jejunal atresia (defined as a mucosal web at the duodenojejunal junction or within 15 cm of the ligament of Treitz), emphasizing anatomic location, clinical presentation, surgical management, and outcomes (Table 1) [6–15]. As summarized in Table 1, these cases demonstrate heterogeneous clinical findings and variable operative strategies, underscoring the need for individualized surgical decision-making, as illustrated by our case. Clinical presentation largely depends on the degree of luminal obstruction. Complete webs typically present early with persistent bilious vomiting, whereas fenestrated webs may result in delayed or intermittent symptoms [10]. Radiologic evaluation may be inconclusive when distal bowel gas is present, highlighting the importance of correlating imaging findings with clinical suspicion. Standard management for duodenal webs consists of duodenotomy with web excision and transverse closure [2]. However, this approach may be suboptimal for lesions located at or just distal to the duodenojejunal junction, particularly in the presence of marked luminal discrepancy. In such cases, segmental resection with primary jejunojejunal anastomosis offers distinct advantages, including restoration of luminal continuity, reduced anastomotic tension, and a lower risk of postoperative stricture. This strategy was therefore appropriate for our patient and resulted in an excellent outcome.
Reported pediatric cases/series of proximal/high type I jejunal atresia (mucosal web).
| Author (year) | Distance from Treitz/ DJ junction | Web type | Key imaging findings | Surgical procedure | Outcome |
|---|---|---|---|---|---|
| Wong et al. (2024) | 15 cm distal to the ligament of Treitz | Fenestrated | Partial proximal small bowel obstruction on contrast study | Segmental resection + end-to-end anastomosis | Good recovery; normal growth at 12 months |
| Diposarosa et al. (2024) | 12 cm distal to the ligament of Treitz | Multiple webs (type I) | Severe proximal dilatation | Resection + anastomosis/web excision + jejunoileoplasty | Both patients died (POD 2 and POD 21) |
| Xiong et al. (2024) | ≤10 cm from the ligament of Treitz (definition used) | Not specified | Not specified (registry-based cohort) | Predominantly resection + anastomosis | Higher NEC risk in the proximal group |
| Jeon et al. (2023) | DJ junction or ≤ 10 cm from Treitz | Type I in 3/7 cases | “Triple-bubble” sign on plain radiographs | Primary anastomosis | All tolerated oral feeds; no major complications |
| Khoei et al. (2021) | Proximal jejunum (distance not specified) | Fenestrated | CT: proximal jejunal obstruction | Web excision | Uneventful recovery |
| Abadi et al. (2021) | At the DJ junction/very proximal jejunum | Multiple webs | Upper GI obstruction | Web excision + jejunojejunostomy (Kimura) | Discharged without complications |
| Sharma et al. (2017) | Jejunum (distance not specified) | Fenestrated | Subacute obstruction; central web perforation | Web excision | Good postoperative course |
| Rajendran et al. (2014) | 10 cm distal to the ligament of Treitz | Complete | Contrast study: upper jejunal obstruction | Resection + end-to-end anastomosis | Favorable recovery |
| Luo et al. (2010) | ≤10 cm from the ligament of Treitz | Not specified | High small bowel obstruction | Duodenal derotation + tapering jejunoplasty + anastomosis | Feeding was tolerated within 14 days |
| Pandey et al. (2008) | ~15 cm distal to the DJ flexure | Complete | Proximal bowel dilatation | Resection + end-to-end anastomosis | Uneventful recovery |
DJ, duodenojejunal.
Conclusion
In conclusion, congenital intrinsic proximal jejunal obstruction caused by a mucosal web near the duodenojejunal junction is a rare and diagnostically challenging condition. A careful radiologic evaluation, exclusion of malrotation, and meticulous intraoperative assessment are essential for accurate diagnosis. Segmental resection with primary anastomosis is a safe and effective surgical option in cases with significant luminal disparity. Early recognition and prompt surgical management are associated with excellent postoperative outcomes.
Acknowledgements
The authors would like to thank the Qatar National Library (QNL) for covering the article processing fee.
Conflicts of interest
The authors declared no potential conflicts of interest.
Funding
None declared.
Ethical considerations
Institutional Review Board (IRB) approval was not required for this case study according to our institution’s ethics committee, as it included a retrospective review of clinical data without identifiable patient information. Informed consent for publication was obtained from the newborn’s parents. The study was conducted in accordance with the principles of the Declaration of Helsinki.

{kind=link}
{kind=link}