





Abstract
Eagle’s Syndrome is a rare condition caused by a particularly elongated styloid process or ossification phenomena of the styloid ligament. It shows up with a triad of symptoms characterized by a sensation of a foreign body in the throat, dysphagia, and unilateral neck-facial. Case 1: A 43-year-old man with right lateral cervical pain and dysphagia underwent styloidectomy using a transoral approach. Case 2: 71-year-old man with right lateral cervical pain, tongue motility deficit, and dysphagia, who underwent styloidectomy using a transcervical approach. The surgery was performed using the VITOM 3D exoscope. The two approaches are both practical. The transoral approach, when feasible, is used to minimize surgical times and postoperative complications. The transcervical approach allows for excellent visualization of the anatomical structures. Moreover, this article aimed to document our experience using a 3D VITOM exoscope, which provides significant advantages in both transoral and transcervical approach.
Introduction
Eagle’s syndrome is a rare condition caused by a particularly elongated styloid process or ossification phenomena of the styloid ligament [1, 2]. It shows up with a triad of symptoms characterized by a sensation of a foreign body in the throat, dysphagia, and unilateral neck-facial pain due to the involvement of V, VII, IX, and X cranial nerves; sometimes, there may be ear pain, tinnitus, odynophagia, generalized head and neck pain, syncope, and transient ischemic attacks [3–5].
The syndrome is challenging to diagnose due to its nonspecific symptoms, resulting in an underestimated prevalence in the population [5]. A clinical presentation and an accurate radiological study are essential for correct interpretation [6]. The most commonly proposed curative treatment is styloidectomy, which allows complete resolution of symptoms in most cases. This procedure can be performed via a transoral or transcervical approach [7, 8].
This article documents our experience with both approaches using a 3D VITOM exoscope.
Case series
Case 1
A 43-year-old man suffering from arterial hypertension, with a story of recurrent episodes of tonsillitis, presented with right cervical pain for a few years and dysphagia for solid foods for three months. Symptoms persist despite medical therapy.
At the ENT physical examination, tenderness on palpation was noted at the right fossa tonsillar area level. An accurate preoperative radiological study revealed an elongated styloid process (Fig. 1).
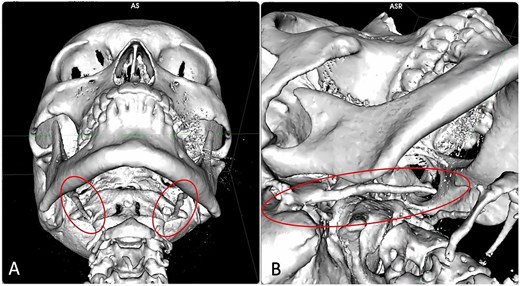
Computed tomography (CT) scan with 3D reconstruction of bilateral elongated styloid process in the 43-year-old patient.
This patient underwent styloidectomy with a transoral approach using the VITOM 3D exoscope (Fig. 2).
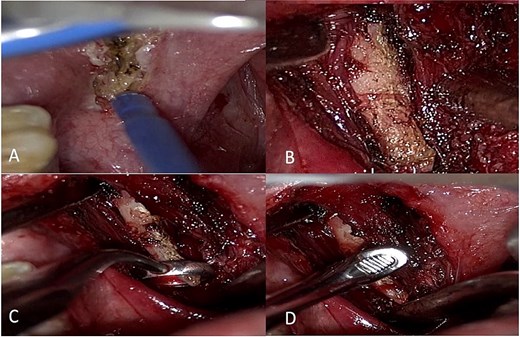
Intraoperative view through VITOM in the transoral approach using mouth distractor, incision along the palatine pillar (A), skeletonization of the styloid process and detachment from the ligaments (B and C), removal in the proximal portion with a Citelli rongeur (D).
Under general anesthesia, an incision was made with monopolar forceps at the level of the right anterior palatine pillar. The mucosal and submucosal planes were detached, and the superior constrictor muscle of the pharynx was incised. The right parapharyngeal space was accessed, and the elongated styloid process was seen. The dissection of the periosteum was then performed, and, using a small ring curette, the styloid process was isolated, freeing it from the aponeurotic insertions.
The osteotomy of the proximal portion of the styloid process was carried out using a Citelli rongeur, respecting the adjacent vascular-nervous structures. Accurate hemostasis with bipolar forceps was performed. The incision was then closed with 3–0 Chromic in a running locking fashion.
The patient reported alleviation of symptoms shortly after and also at his three-month post-operative visit.
Case 2
A 71-year-old man with diverticular disease and prostatic hypertrophy. For the last two years, he reported right-sided cervical pain associated with lingual motility deficit, dysphagia, pharyngodynia, and reflex otalgia. He underwent corticosteroid therapy with partial benefit.
The computed tomography scan showed a prominent aspect of the proper styloid process with ossification of the stylohyoid ligament and an intimate relationship with the external carotid artery branches (Fig. 3).
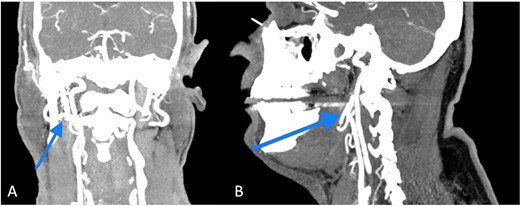
The CT scan showed a prominent aspect of the right styloid process with ossification of the stylohyoid ligament, an intimate relationship with the branches of the external carotid artery was also present.
This patient underwent styloidectomy with a transcervical approach using the VITOM 3D exoscope (Fig. 4).
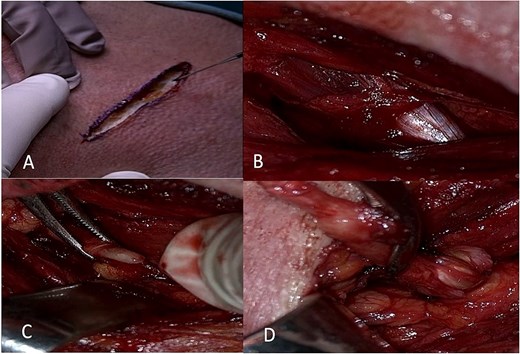
Intraoperative view starting from skin incision (A) in the anterior border of the sternocleidomastoid muscle, the localization of the digastric muscle and tendon (B), skeletonization of the styloid process (C), followed by removal after fracture of the styloid process.
Under general anesthesia, a skin incision was made 4 cm from the lower edge of the mandible on the right. The subcutaneous incision was performed, and an upper and lower myocutaneous flap was prepared. The anterior border of the sternocleidomastoid muscle was exposed and isolated, followed by the posterior belly of the digastric. The internal jugular vein was identified. The right styloid process was accurately depicted, separated from the stylohyoid musculature, and dislocated and fractured at the proximal portion. It was then removed, preserving the adjacent vascular and nervous structures. Accurate hemostasis was achieved using bipolar forceps, and a Redon drain was placed. The skin incision was closed with an intradermal suture.
Three months after the operation, the symptoms improved significantly.
Discussion
The styloid process is an elongated, tapered projection that originates in the petrous portion of the temporal bone, lying medially and anteriorly to the stylomastoid foramen, between the internal and external carotid arteries, and laterally to the tonsillar fossa. The stylopharyngeal, stylohyoid, and styloglossal muscles are attached to the styloid process. This bony process supports the stylohyoid and stylomandibular ligaments. The stylohyoid ligament connects the apex of the styloid process and the lesser horn of the hyoid bone, and the stylomandibular ligament extends from the styloid process to the parotid masseteric fascia between the mastoid process and the mandible [4].
Watt W. Eagle first described Eagle’s syndrome in 1937, discussing the combination of pain associated with an abnormal stylohyoid complex. It is a rare condition caused by a particularly elongated styloid process or ossification phenomena of the styloid ligament [9, 10].
Murtagh et al. explained that Eagle’s syndrome symptoms stem from its pathophysiology, which includes (i) the theory that traumatic fracture of the styloid process with a proliferation of granulation tissue can apply pressure on the surrounding area; (ii) compression of the glossopharyngeal nerve, the mandibular branch of the trigeminal, or the chorda tympani; (iii) the theory of insertion tendonitis due to inflammation of the tendinous part of the stylohyoid insertion; (iv) irritation of the pharyngeal mucosa by direct compression or post-tonsillectomy scarring (with involvement of cranial nerves V, VII, IX, and X); and (v) the theory of irritation of the sympathetic nerves surrounding the carotid vessels [6].
Eagle’s syndrome presents with a triad of symptoms characterized by a sensation of a foreign body in the throat, dysphagia, and unilateral neck-facial pain due to the involvement of V, VII, IX, and X cranial nerves; sometimes, there may be ear pain, tinnitus, odynophagia, generalized head and neck pain, syncope, and transient ischemic attacks [3–5].
Due to its nonspecific symptoms, the syndrome is challenging to diagnose, resulting in an underestimated prevalence in the population. A clinical presentation and an accurate radiological study are essential for precise interpretation [6].
The most proposed curative treatment is styloidectomy, which allows complete resolution of symptoms in most cases [11, 12]. This procedure can be performed via a transoral or transcervical approach [4].
The two approaches are both practical [3]; the transoral approach, where possible, may reduce surgical times and post-operative complications. This approach is suitable for aesthetic consideration, as external scarring is avoided, and for shorter operative times. Nevertheless, exposure of the retropharyngeal spaces to intraoral contents increases the risk of infection. The intraoral approach also has the disadvantages of poor access, as in cases of trismus, and risk of intraoperative injury [11–13]. The transcervical route allows for excellent visualization of the vessels and enables us to appreciate macroscopically the effectiveness of the vascular-nervous decompression. However, it requires a more extended surgery, resulting in a visible scar [4].
This article aimed to document our experience with both these approaches using a 3D VITOM exoscope. In both cases, the VITOM 3D system enabled the surgeon to work comfortably, offering good ergonomics for the surgical staff and providing 3D high-definition images of the surgical field, ensuring enhanced magnified visualization of even small anatomical structures, which are particularly useful for training residents. Moreover, the use of VITOM 3D exoscope has been reported to reduce operative times compared to conventional surgical tools like endoscope or microscope [14]. These findings support the use of the 3D exoscope for both types of surgical approaches, although additional data would be beneficial to confirm our findings.
The two approaches are effective; the transoral approach, when possible, reduces surgical times and post-operative complications. The transcervical approach allows for excellent visualization of the vessels and enables us to appreciate macroscopically the efficacy of the vascular-nervous decompression. Moreover, 3D VITOM can be a very useful tool in both approaches.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}