





Abstract
Perilunate fracture-dislocations (PLFDs) are rare but severe wrist injuries. Median nerve involvement is common, whereas ulnar nerve injury is exceptionally rare. Delayed diagnosis remains frequent and negatively impacts outcomes. A healthy 30-year-old man sustained a fall onto his outstretched left hand, presenting with wrist deformity and ulnar sensory deficit. Radiographs showed disrupted Gilula’s lines and a scaphoid waist fracture consistent with PLFD. Closed reduction failed, and open reduction with internal fixation via combined volar and dorsal approaches was performed, including carpal tunnel release, scaphoid fixation, ligament repair, and Kirschner wire stabilization. Postoperatively, ulnar sensation improved and carpal alignment was maintained, but scaphoid nonunion developed. The final Mayo Wrist Score was 75. PLFDs with ulnar nerve injury pose diagnostic and therapeutic challenges. Early comprehensive surgical management is essential, though complications may still occur, necessitating long-term follow-up.
Introduction
Perilunate fracture-dislocations (PLFDs) are rare but severe wrist injuries, accounting for approximately 7%–10% of carpal traumas. They typically occur in young adults following high-energy mechanisms such as falls or motor vehicle accidents. The classic injury mechanism involves axial loading of a hyperextended, ulnarly deviated wrist with intercarpal supination, leading to perilunate instability and frequently an associated scaphoid fracture [1]. Patients usually present with wrist pain, swelling, and restricted motion; however, subtle clinical findings and the complexity of these injuries contribute to misdiagnosis or delayed diagnosis in up to 25% of cases. Early recognition is critical, as delayed treatment increases the risk of chronic pain, post-traumatic arthritis, and functional impairment. Plain radiographs remain the initial diagnostic modality, while computed tomography is valuable for characterizing fracture patterns and surgical planning. Scaphoid fractures accompany more than half of perilunate dislocations, necessitating meticulous evaluation. Although closed reduction may be attempted initially, unsuccessful cases require urgent open reduction with internal fixation and ligament repair. Surgical intervention within two months is associated with improved outcomes, although acceptable results have been reported following delayed treatment [2].
Neurological complications most commonly involve the median nerve, resulting from edema, hematoma, or direct compression. Ulnar nerve involvement is uncommon and typically associated with complex injury patterns [2]. When neurological deficits are present, early surgical decompression is recommended to optimize recovery [3]. Scaphoid nonunion represents another significant complication, often related to vascular compromise and treatment delay; combined scaphoid fixation and ligament repair improves union rates and carpal stability [4].
Surgical management focuses on anatomical reduction, fracture fixation, and ligament repair. Volar and dorsal approaches offer complementary advantages, and combined approaches may be necessary in complex cases [1]. This report describes a rare PLFD complicated by ulnar nerve sensory deficit and subsequent scaphoid nonunion despite timely surgical intervention, highlighting the diagnostic challenges and potential complications associated with these injuries.
Clinical presentation
A 30-year-old healthy male with no prior medical or surgical history sustained a fall of approximately 2 m from a ladder, landing on his outstretched left hand. He was initially managed at a local hospital and subsequently transferred to our facility for specialist care. On arrival, examination revealed visible deformity, abrasions, swelling, and generalized tenderness of the left hand and wrist. Wrist range of motion was restricted due to pain. Radial and ulnar pulses were palpable; however, there was reduced sensation and impaired two-point discrimination over the ulnar aspect of the hand.
Plain radiographs demonstrated disrupted Gilula’s lines, loss of collinearity between the radius and lunate, and a fracture through the scaphoid waist (Fig. 1). Closed reduction under sedation was attempted in the emergency department but was unsuccessful. A below-elbow cast was applied, and the patient was taken to the operating theater for open reduction and internal fixation.

Preoperative radiographs (PA, LAT) of the left wrist demonstrating disrupted Gilula’s lines, carpal malalignment, and a scaphoid waist fracture consistent with perilunate fracture-dislocation.
An extended carpal tunnel approach was performed, allowing carpal tunnel release and reduction of the lunate. The dorsal scapholunate interosseous ligament was intact, and the volar lunotriquetral ligament was repaired. Through a universal dorsal approach, the scaphoid was fixed with a headless screw (Fig. 2). Percutaneous Kirschner wires were inserted across the triquetrum–capitate and lunotriquetral joints, as well as for the radial styloid fracture (Fig. 3).
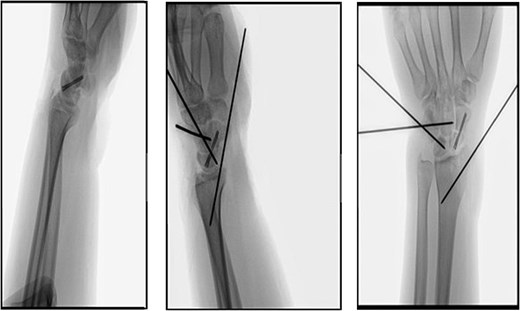
Intraoperative fluoroscopic views (PA, LAT) showing anatomic reduction with headless screw fixation of the scaphoid and Kirschner wires stabilizing the triquetrum–capitate, lunotriquetral, and radial styloid joints.

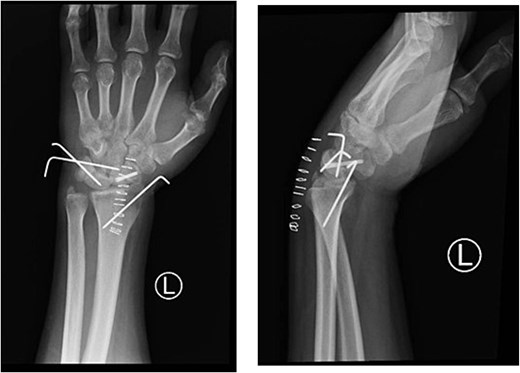
Immediate postoperative radiographs (PA, LAT) demonstrating restored carpal alignment following open reduction, scaphoid screw fixation, ligament repair, and Kirschner wire stabilization.
Postoperatively, sensation improved, and the wrist was immobilized in 20° of extension with a volar slab for 8 weeks. Following K-wire removal, the slab was replaced with a removable splint, completing 12 weeks of immobilization (Figs 4 and 5). Final radiographs showed normal carpal alignment and satisfactory screw positioning (Fig. 6). The patient subsequently developed scaphoid nonunion and elected to undergo a salvage procedure at a later date. At follow-up, the Mayo Wrist Score was 75, indicating a fair outcome with moderate functional limitation.
Four-week postoperative radiographs (PA, LAT) showing maintained carpal alignment with headless screw fixation of the scaphoid and Kirschner wires in situ.
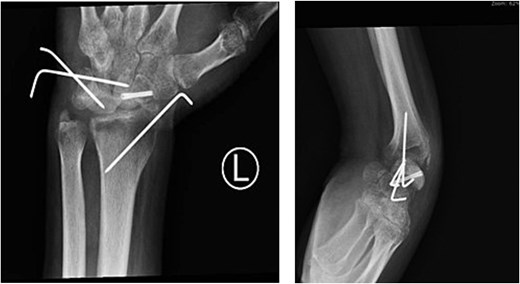
Six-week postoperative radiographs (PA, LAT) demonstrating preserved carpal alignment with the scaphoid screw and Kirschner wires in situ.
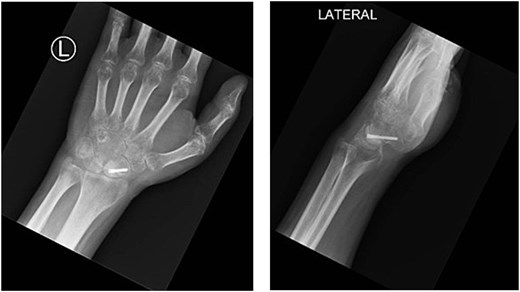
Final follow-up radiographs (PA, LAT) showing maintained carpal alignment with a retained headless screw in the scaphoid following Kirschner wire removal.
Discussion
In this review, we identified nine published cases of perilunate dislocations (PLDs) and perilunate fracture-dislocations (PLFDs) associated with ulnar nerve injury reported over a 60-year period (Table 1). All patients were male, and injuries predominantly involved the left, non-dominant hand. Patient age ranged from 20 to 58 years. PLFDs accounted for the majority of cases (eight of nine), while isolated PLD was reported in only one case. Associated injuries were common, including distal radius or radial styloid fractures in six cases and carpal fractures in three. Concomitant median nerve injury was reported in one patient, and open fractures occurred in two cases. These findings indicate that ulnar nerve involvement is more frequently associated with complex PLFD patterns rather than isolated ligamentous dislocations [5–7].
Summary of nine published cases of perilunate dislocations (PLDs) and perilunate fracture-dislocations (PLFDs) associated with ulnar nerve injury, reported over a 60-year period
| Gender | Age | Side | Type of injury | Mechanism of injury | Median nerve injury | Ulnar nerve injury | Associated fractures (scaphoid, lunate, capitate) | Associated injures | Management | Outcome (ROM, function, pain, deformity) | Follow up Period | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | 34 | Left/not dominant | PLFD (trans-scaphoid, transcapitate, and perilunate fracture-dislocation) | MVA, a motorcycle collision | No | Yes | Distal radius rim, scaphoid, and capitate fractures | Ulnar and median nerves neuropraxia | ORIF, k wires for transscaphoid fracture, plate fixation of the transcapitate, ulnar nerve decompression | FROM + 100% function + no pain | 3 months | Avendano JP, Gallagher DO, Van Kouwenberg E (2023) [8] |
| Male | 39 | Left/not dominant | PLFD (lunate dislocation with an avulsion fracture of the radial styloid and ulnar styloid process) | Fell from tree on extended hand | Yes | Yes | Radial styloid and ulnar styloid process fracture | Tinel’s sign, finger clawing | ORIF, Kirschner wire, and a volar locking plate, ulnar nerve decompression with ligament repair | Mild ROM limitation + 100% function + no pain | 1 year | Yamada K, Sekiya S, Oka S, Norimatsu H (1995) [7] |
| Male | 36 | Left/not dominant | PLFD (volar dislocation of the lunate associated with scaphoid and distal radial fractures) | MVA, falling from his motorcycle | No | Yes | Scaphoid and radial styloid fracture | Ulnolunate ligamentous disruption | ORIF, K-wires for lunate, screw for radial styloid, ligament repair, decompression of Guyon’s canal | FROM + 100% function + no pain | 3 months | Shariff Z, et al. (2009) [9] |
| Male | 27 | Right/dominant | PLD (hamate and pisiform dislocation) | Crushed his hand and wrist in a rolling press | No | Yes | Third metacarpal shaft fracture | Open wound, severe splitting of the hypothenar muscle | ORIF, hamate and pisiform were reduced by Kirschner wire + dorsal plate | FROM, 50% function (reduced grip strength), mild pain | 6 months | Matsumoto T, et al. (2005) [10] |
| Male | 33 | Left/not dominant | PLFD (trans-scaphoid perilunate) | Falling 2 m from a scaffold | No | Yes | Scaphoid fracture | Claw deformity and ulnar artery thrombosis | ORIF, cannulated screw for scaphoid, K-wire for lunotriquetral joint, artery repair | FROM + 100% function + no pain | 5 months | Imao K, et al. (2016) [11] |
| Male | 43 | Left/ not dominant | PLFD (radial perilunate dislocation) | MVA, running his motorcycle off the road and into a ditch | No | Yes | Radial styloid process fracture | stiffness | ORIF, with volar plate, Kirschner wire, ligament repair | FROM + 100% function + no pain | 1 year | Sagini D, et al. (2011) [12] |
| Male | Mid 20s | Left/not dominant | PLFD (comminuted, intra-articular distal radius fracture with dislocation of the radiocarpal joint) | MVA | No | Yes | Distal radius (intra-articular) | Ring- and small-finger clawing | External fixator, percutaneous pins, ulnar nerve grafting (sural nerve) | Restricted ROM and function (Persistent clawing and sensory deficits) | 1 year 4 months | Wilson CJ, et al. (2008) [13] |
| Male | 20 | Left/not dominant | PLFD (dorsal radiocarpal dislocation with a comminuted fracture of the radial styloid and an avulsed ulnar styloid) | Forced dorsiflexion by the back of a military truck which was attempting to park | No | Yes | Radial and ulnar styloid | Open wound | ORIF, k wires, “figure-8” tension band wire, ligament repair | FROM + 100% function + no pain | 1 year | Fernandez DL (1981) [14] |
| Male | 58 | Right/dominant | PLD (peri-triquetral lunate dislocation) | Slipped off a kerb falling onto outstretched hand | No | Yes | None | None | Closed reduction under GA | FROM + 100% function + no pain | 3 months | Bollen SR (1988) [15] |
PLDs and PLFDs result from high-energy trauma applied to a hyperextended, ulnarly deviated wrist with intercarpal supination [16, 17]. Common mechanisms include motor vehicle collisions, crush injuries, and military training accidents [18]. Injury patterns are classified as lesser arc, greater arc, and inferior arc. Lesser arc injuries are purely ligamentous, whereas greater arc injuries involve associated fractures, most commonly of the scaphoid. Inferior arc injuries transmit force through the radiocarpal joint and frequently involve the radial styloid [17, 19, 20].
Accurate diagnosis requires a high index of suspicion and thorough neurovascular examination, as delayed or missed diagnosis is associated with chronic pain, instability, and permanent neurological deficits [9, 21]. While plain radiographs are usually diagnostic, CT and MRI provide superior assessment of fracture morphology and ligamentous injury [22]. Missed injuries often progress to chronic disability and may necessitate salvage procedures with inferior outcomes [2].
Management remains challenging due to injury rarity and the absence of standardized protocols [23]. Closed reduction may temporarily restore alignment and decompress neural structures but rarely maintains stability, with high rates of redislocation and suboptimal outcomes [24]. Consequently, open reduction and internal fixation (ORIF) is recommended, particularly in cases with associated nerve injury [5, 25]. ORIF allows restoration of carpal alignment, fracture fixation, and ligament repair. Early intervention—ideally within 7 days—yields superior outcomes, whereas delays beyond 6 weeks increase the risk of nonunion, stiffness, and post-traumatic arthritis [10, 26, 27].
Various fixation techniques have been described, including K-wires, screws, and external fixation [28]. In complex cases, combined volar and dorsal approaches provide complementary advantages, allowing nerve decompression, improved visualization, and stable fixation [5, 25]. Scaphoid nonunion remains a recognized complication influenced by fracture displacement, vascular compromise, and timing of surgery [4, 11]. Combining scaphoid fixation with ligament repair improves union rates and carpal stability [13]. Long-term follow-up is essential, as degenerative changes may develop despite appropriate management [2].
Conclusion
This case highlights the importance of early recognition and prompt surgical management of perilunate fracture dislocations, particularly when associated with scaphoid fractures and neurological deficits. Combined surgical approaches may be necessary to achieve adequate decompression, reduction, and fixation. Despite timely and comprehensive treatment, complications such as scaphoid nonunion can still occur, underscoring the complexity of these injuries. Clinicians should remain vigilant for late sequelae, ensure long-term follow-up, and counsel patients about the possibility of additional procedures. Ultimately, this case reinforces that even in optimal settings, PLFDs remain high-risk injuries with variable outcomes.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}