





Abstract
Vertebrobasilar dolichoectasia (VBD) is a rare clinical condition that occasionally causes secondary trigeminal neuralgia through compression of the trigeminal nerve. Reported treatment methods include oral carbamazepine, microvascular decompression, percutaneous balloon compression, and gamma knife radiosurgery; however, outcomes are often limited, and symptom recurrence is common. Moreover, many of these therapeutic approaches are associated with significant adverse effects. In June 2025, a 66-year-old man presented with VBD-induced secondary trigeminal neuralgia. His diagnosis was confirmed through imaging and clinical studies upon admission. The patient was treated by placing a flow-diverting stent in one vertebrobasilar artery and occluding the contralateral vertebral artery, to reconstruct the blood flow and reduce compression of the trigeminal nerve. The surgical outcome was favorable, with no painful attacks and a visual analogue scale pain score of 0 by postoperative Day 6.
Introduction
Vertebrobasilar dolichoectasia (VBD) is characterized by the expansion, elongation, and tortuosity of the basilar or vertebral artery. In VBD, vascular displacement can lead to nerve compression. Compression of the trigeminal nerve can result in trigeminal neuralgia, a painful condition that features repeated, sudden electric shock-like or stabbing pain in areas innervated by the trigeminal nerve [1].
Traditional treatments of VBD-induced trigeminal neuralgia, including various medications and surgeries [2–5], are not always effective and carry associated risks [6–11]. Interestingly, a recent attempt to treat VBD using a stent and embolization coil resulted in the incidental relief of trigeminal neuralgia; however, details regarding stent and coil placement were scarce, and the patient experienced left-sided facial palsy and reduced right limb muscle strength [12]. To date, no studies have intentionally targeted trigeminal neuralgia secondary to VBD using endovascular techniques. Here, we report the directed use of endovascular treatment to address VBD-induced trigeminal neuralgia, providing detailed procedural insights and pain-related outcomes.
Case report
A 66-year-old man was admitted with a 10-month history of severe left facial pain, which had worsened over the past day, impaired mental status, and deteriorating general condition. The pain was localized to the left maxillary region and lateral orbit. Talking, drinking, and washing his face all triggered attacks. The pain was described as sharp, knife-like, and electric shock-like.
At onset, oral carbamazepine was effective in reducing pain intensity; however, as the condition progressed, pain episodes became more frequent and resistant to medication. The patient had a 10-year history of hypertension, managed with perindopril tert-butylamine, and a history of coronary artery disease.
Upon admission, the patient underwent head and neck computed tomography angiography (CTA), magnetic resonance imaging (MRI), and digital subtraction angiography (DSA) (Fig. 1). The findings were as follows: basilar artery diameter > 4.5 mm; bifurcation level at the third ventricle (Grade 2); horizontal bending reaching the left cerebellopontine angle (Grade 3); left trigeminal nerve compressed and deformed by the ectatic vertebrobasilar artery; and neurovascular conflict (Grade 5).
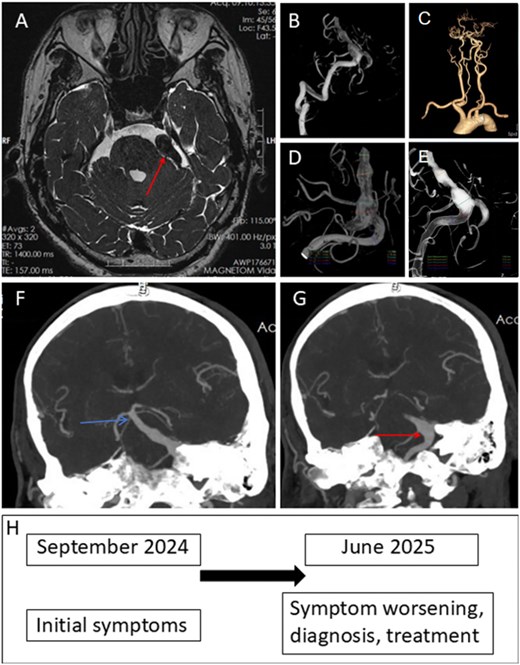
Patient met the diagnostic criteria for vertebrobasilar artery dilation. (A) Non-contrast MRI shows a dilated vertebrobasilar artery located in the left cerebellopontine angle. The left trigeminal nerve is compressed and deformed by the dilated vertebrobasilar artery. Vascular compression is grade 5. (B) Three-dimensional (3D) DSA demonstrates overall tortuous dilatation of the vertebrobasilar artery. (C) CTA reconstruction of the head and neck vessels shows tortuous dilatation of the vertebrobasilar artery, with the vertebrobasilar system shifted to the left. (D) 3D angiography via the left vertebral artery shows that the dilated vertebrobasilar artery is mainly located at the distal right vertebral artery and the proximal basilar artery. There is no obvious dilatation at the distal end of the left vertebral artery. The maximal basilar artery diameter is >4.5 mm. (E) 3D angiography via the right vertebral artery shows that the dilated vertebrobasilar artery is mainly located at the distal right vertebral artery and the proximal basilar artery. There is no obvious dilatation at the distal end of the left vertebral artery. The maximal basilar artery diameter reaches 9 mm. (F) CTA shows that the basilar bifurcation reaches the floor of the third ventricle. (G) CTA shows that the basilar artery deviates from the midline and is located at the internal auditory canal; the transverse kinking/displacement of the basilar artery is in the left cerebellopontine angle (grade 3). (H) Patient timeline, from initial symptoms to treatment.
In preoperative physical examinations, the patient had a Barrow Neurological Institute pain intensity score of V and a visual analogue scale score of 10. Pain frequency was >20 times per day and was triggered at any time.
On the basis of imaging and clinical information, the patient was diagnosed with VBD with secondary trigeminal neuralgia, as well as hypertension. The patient refused craniotomy and microvascular decompression. Percutaneous trigeminal balloon compression was considered, but this technique is associated with a high risk of recurrence [11]. It was therefore decided that the patient would undergo flow-diverting stent placement in one vertebrobasilar artery with contralateral vertebral artery occlusion. Following a comprehensive risk–benefit assessment, the procedure was approved by the institutional ethics committee, and written informed consent was obtained from the patient.
To prepare for surgery, the patient received oral aspirin (100 mg) and clopidogrel (75 mg) once daily for 5 days to reduce perioperative thrombosis risk and ensure stent patency. The procedure was performed with the patient in a supine position under general anesthesia. For stent placement, the right radial artery was punctured and fitted with a 6-French (Fr) thin-walled radial sheath. Simultaneously, the right femoral artery was punctured and fitted with an 8-Fr femoral sheath for the occlusion procedure. Full cerebral angiography was performed via the femoral artery.
Via the right radial sheath, a distal access catheter was advanced through the upper limb artery, right subclavian artery, and right vertebral artery to the V3 segment. An XT27 stent delivery microcatheter was then inserted through the distal access catheter and guided by a 0.014-inch microwire to the P2 segment of the right posterior cerebral artery. Next, a Nuva flow-diverting stent (model TJED-D-6.5-35) was released through the XT27 catheter (Fig. 2). Once the stent is released, it can be extended to a length of 56 mm within a 6.0-mm-diameter blood vessel, according to the manufacturer. Thus, a single 35-mm device was sufficient to cover the clinically relevant ectatic segment while ensuring safe distal and proximal landing zones. The distal landing zone of the flow-diverting stent was located at the distal basilar artery, approximately 0.8 mm from the origin of the superior cerebellar artery; the proximal end of the stent was positioned within the proximal V4 segment of the vertebral artery, about 2 cm proximal to the dural ring.
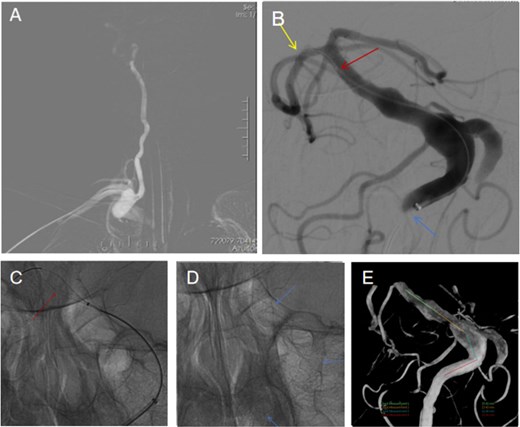
A flow-directing close-mesh stent was implanted from the right vertebral artery to the basilar artery (A) Angiography was performed through the right vertebral artery, and a flow-diverting dense-mesh stent was deployed. (B) Contrast image during the procedure showing the guidewire in the right posterior cerebral artery (yellow arrow); the tip of the stent catheter at the distal basilar artery (red arrow), which is also the distal landing point of the flow-diverting stent (red arrow); and the 5F distal access catheter at the distal vertebral artery (blue arrow). (C) Intraoperative findings. The leading end of the stent was opened through the XT27 stent catheter. (D) Cardiography after stent release shows deployment of the Nuva 6.5 × 35 (extendable to 56 mm) flow-diverting dense-mesh stent via the stent catheter (blue arrow). (E) On the basis of 3D vascular reconstruction, the expected coverage of the vertebrobasilar segment was 15.42 + 13.43 + 11.48 + 13.91 = 54.24 mm.
Via the femoral sheath, an 8-Fr guiding catheter was positioned in the left subclavian artery. Through this, a 5-Fr distal access catheter was advanced, followed by the insertion of an SL-10 microcatheter. The microcatheter was positioned at the junction of the distal left vertebral artery and the basilar artery, and a coil was released to occlude the artery (Fig. 3).
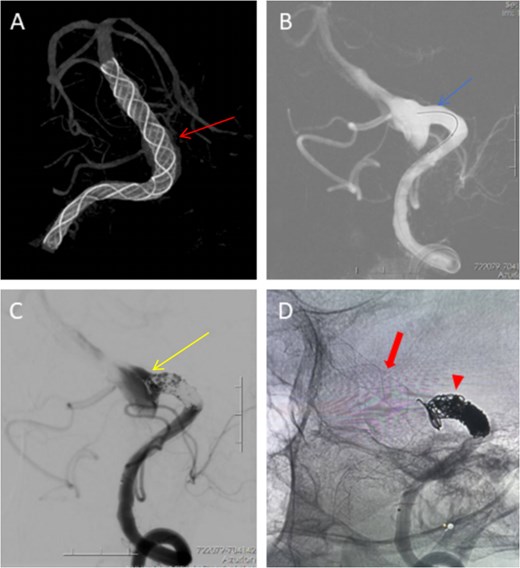
Occlusion of the left vertebral artery. (A) VAsa computed tomography reconstruction after stent release shows that the stent (red arrow) was satisfactorily deployed, covering the elongated, dilated vertebrobasilar artery. (B) Through a femoral arterial sheath, an 8F guiding catheter was inserted and positioned in the left subclavian artery. Through the guiding catheter, a 5F distal access catheter was advanced, and through the distal access catheter, an SL-10 microcatheter was advanced and positioned at the junction of the distal left vertebral artery and the basilar artery (blue arrow). (C) Left vertebral artery angiography after spring coil embolism shows decreased blood flow in the direction of the vertebrobasilar artery. (D) Using non-decimation technology, the relationship between the flow-diverting dense-mesh stent (red arrow) and the coils (triangular arrow) is shown. The coils were outside the stent, thereby reducing the impact of the flow from the left vertebral artery direction into the ectatic segment.
Intraoperatively, systemic heparinization (4000 units) was administered. Tirofiban was infused at 3 mL/h, 0.075 μg/kg/min, during surgery and for 48 h postoperatively to prevent clotting; the dose was then adjusted to 2 mL/h, 0.05 μg/kg/min, for 24 h before being discontinued. Postoperatively, the patient continued to receive oral aspirin (100 mg/day) and clopidogrel (75 mg/day) for 180 days, followed by enteric-coated aspirin (100 mg/day) for 365 days.
Following the surgery, the patient experienced marked pain relief (Table 1) and improved mental status. He was able to speak and eat without triggering pain. To systematically evaluate potential neurological complications, standardized neurological examinations were performed immediately after the procedure, daily during hospitalization, and at follow-up assessments. Although postoperative angiography confirmed stent patency and preservation of perforator vessels, the absence of diffusion-weighted magnetic resonance imaging cannot completely exclude clinically silent infarction. The patient has been advised to undergo a follow-up MRI in the near future and the results will be reported in a follow-up.
Preoperative and postoperative VAS pain score.
| Time point | VAS score | Attack frequency |
|---|---|---|
| Preoperative | 10 | Triggered any time, >20 times/day |
| Postoperative Day 1 | 6 | >20 times/day |
| Postoperative Day 2 | 3 | 5–10 times/day |
| Postoperative Day 3 | 2 | ~5 times/day |
| Postoperative Days 4–5 | 2 | ~5 times/day |
| After postoperative Day 6 | 0 | No episodes |
| After postoperative Day 60 | 0 | No episodes |
Abbreviation: VAS, visual analogue scale; 10 = highest level of pain, 0 = no pain.
Discussion
Although VBD-induced trigeminal neuralgia has been treated with carbamazepine [2], microvascular decompression [3], percutaneous balloon compression [4], and gamma knife radiosurgery [5], these treatments can be problematic. With oral carbamazepine, both treatment resistance and adverse effects are common [6]. Microvascular decompression is considered the gold-standard surgical option [7] but is technically challenging, invasive, and requires craniotomy, which some patients refuse [7]. Microvascular decompression also carries risks such as postoperative hypertension and hearing loss [8, 9], and craniotomy is associated with neurological complications [10]. Balloon compression and stereotactic radiosurgery techniques such as gamma knife surgery are less invasive; however, their long-term efficacy is limited [11], and stereotactic radiosurgery is associated with postoperative facial numbness [11].
Flow-diverting stent implantation combined with contralateral vertebral artery occlusion is minimally invasive and does not require craniotomy. It is widely used to treat vertebral [13] and basilar [14] artery aneurysms and has also been reported as a treatment for VBD [15]. Nevertheless, this strategy entails non-trivial risks, including posterior circulation ischemia, perforator infarction, in-stent thrombosis, and haemorrhagic complications associated with prolonged dual antiplatelet therapy. Moreover, this approach is not proposed as a first-line treatment, but rather as a highly selective option reserved for patients with refractory symptoms, refusal of or contraindications to craniotomy, and favorable vertebrobasilar anatomy as demonstrated by preoperative angiographic assessment.
This patient presented with severe trigeminal neuralgia secondary to compression of the trigeminal nerve by an enlarged vertebrobasilar artery. Conventional therapeutic modalities proved ineffective, and the patient declined craniotomy. Therefore, the surgical intervention was performed with the aim of altering blood flow dynamics by redirecting vertebrobasilar arterial flow via a flow diverter and occluding the contralateral vertebral artery. This modification reduces the hemodynamic impact and compressive forces exerted on the trigeminal nerve, thereby addressing the trigeminal neuralgia.
Notably, placement of a flow diverter in one vertebral artery may lead to hemodynamic instability, as antegrade flow in the contralateral vertebral artery can impinge on the extradiverter sac cavity. Therefore, simultaneous occlusion of the contralateral vertebral artery is indicated. In the present case, angiographic evaluation demonstrated robust basilar artery opacification via the dominant right vertebral artery, confirming adequate posterior circulation perfusion and thereby reducing the risk of brainstem or cerebellar ischemia. The occlusion site was selected at the junction of the distal vertebral artery and the basilar artery to avoid compromising major branch vessels, including the ipsilateral posterior inferior cerebellar artery. Postoperatively, antiplatelet therapy was administered as a combination of short-term low-dose tirofiban, long-term oral aspirin, and long-term oral clopidogrel. This regimen is designed to prevent and reduce the risk of postoperative perforator artery occlusion events without elevating the risk of bleeding.
Notably, in a recent case of VBD with trigeminal neuralgia, stenting and occlusion to treat VBD was reported to incidentally resolve the patient’s trigeminal neuralgia, although adverse effects were noted [12]. In contrast, in the present case, we performed stenting and occlusion specifically aimed at reducing the trigeminal nerve compression. This technique proved to be a simple and effective solution for the patient’s trigeminal neuralgia and VBD, with no apparent adverse effects.
The present case report has limitations. Only one patient was treated, and the follow-up period was short; future studies involving more patients and a longer follow-up period are warranted. Nonetheless, together with the incidental report by Jing et al. [12], the present case report indicates that endovascular treatment may be a promising therapy for VBD-induced trigeminal neuralgia.
Acknowledgements
We thank Bronwen Gardner, PhD, Katherine Halievski, PhD, and Rachel Baron, PhD, from Liwen Bianji (Edanz) (www.liwenbianji.cn/) for editing a draft of this manuscript.
Conflicts of interest
None declared.
Funding
None declared.

{kind=link}
{kind=link}
{kind=link}