





Abstract
High-energy open tibial fractures with segmental bone loss and extensive soft-tissue necrosis remain limb-threatening, especially when only one recipient artery is patent. We report a 37-year-old man with a Gustilo-Anderson type IIIB open distal tibial fracture, posterior tibial artery injury, a 7-cm tibial defect and a 14 x 25 cm soft-tissue defect after serial debridement. After emergency external fixation and revascularization, the wound was optimized with repeated debridement and circumferential negative-pressure wound therapy. Definitive reconstruction used a vascularized pedicled fibular graft from the injured leg to bridge the tibial defect, combined with a latissimus dorsi free flap for coverage; the thoracodorsal artery was anastomosed end-to-side to the posterior tibial artery under 3D magnification. The flap survived without infection or secondary necrosis, allowing early rehabilitation with stable coverage and maintained alignment.
Introduction
Severe open tibial fractures with segmental bone loss have high risks of infection, non-union, and amputation, particularly when accompanied by arterial injury [1, 2]. Limb salvage requires meticulous debridement, stable fixation, restoration of perfusion, and early durable soft-tissue coverage [3]. When bone loss exceeds 6 cm, vascularized bone transfer provides living cortical bone with intrinsic blood supply, improving biology and resistance to infection [4]. Large lower-leg defects often need free-tissue transfer; the latissimus dorsi provides reliable, broad coverage [5]. When only a single runoff vessel is available, combining a pedicled vascularized fibular graft with a single free flap may reduce microvascular risk. We report a hybrid limb-salvage strategy combining a vascularized pedicled fibular graft with a latissimus dorsi free flap to reconstruct a complex tibial defect after high-energy trauma.
Case report
A 37-year-old man sustained a high-energy open injury to the right lower leg following a traffic accident. Emergency debridement, external fixation and vascular exploration with thrombectomy were performed to restore distal perfusion. Despite stabilization, progressive necrosis developed.
After serial radical debridement, an extensive anteromedial soft-tissue defect (approximately 14 × 25 cm) with exposed tibia and a 7-cm segmental tibial defect remained (Figs 1 and 2). Computed tomography angiography demonstrated occlusion of the anterior tibial artery and distal peroneal artery, leaving the posterior tibial artery as the only functional runoff.

Initial injury and preoperative imaging. (A) Initial presentation of a Gustilo–Anderson type IIIB open fracture of the right tibia. (B) Preoperative anteroposterior radiograph demonstrating a comminuted open tibial fracture with segmental bone loss.
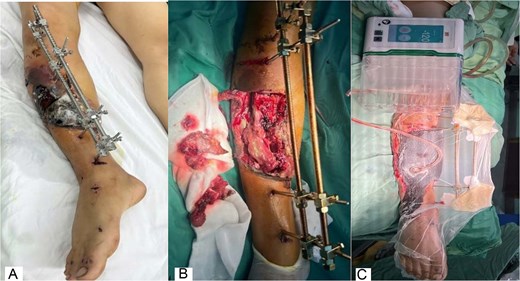
Wound evolution and negative-pressure wound therapy. (A) Post-debridement wound with external fixation in place, showing progressive skin necrosis prior to the second debridement. (B) Intraoperative view after serial debridement demonstrating extensive deep soft-tissue necrosis and an exposed tibial defect. (C) Full-limb continuous negative-pressure wound therapy (CNP 3D easy-dress) applied to enclose the limb and the external fixation frame.
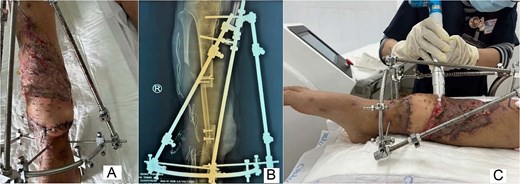
The wound was optimized using repeated debridement and circumferential negative-pressure wound therapy that enclosed the limb and external fixation (Fig. 2C), promoting granulation tissue (Fig. 3A). Definitive reconstruction (6 February 2025) used a vascularized pedicled fibular graft from the injured leg, fashioned to bridge the tibial defect and secured with screws and wires, while the external fixator maintained alignment (Fig. 3B and C).

Wound-bed preparation and bony reconstruction imaging. (A) Granulation tissue formation after serial debridement and continuous negative-pressure wound therapy. (B) Postoperative radiograph showing the vascularized pedicled fibular graft bridging the tibial defect; the external fixator maintained limb stability during recovery. (C) Postoperative three-dimensional computed tomography reconstruction confirming graft position spanning the tibial defect with stabilization by external fixation.
Soft-tissue reconstruction was completed with a latissimus dorsi free flap with a skin paddle. The thoracodorsal artery was anastomosed end-to-side to the posterior tibial artery under 3D magnification (Fig. 4A and B). Split-thickness skin grafting was applied over the muscle flap (Fig. 4C). The frame was modified to a semicircular configuration to improve stability and facilitate postoperative flap care.

Latissimus dorsi free flap transfer. (A) Intraoperative photograph of end-to-side microvascular anastomosis between the thoracodorsal artery and the posterior tibial artery. (B) Harvest of the latissimus dorsi free flap with a skin paddle based on the thoracodorsal vessels. (C) Early postoperative view demonstrating successful coverage of the lower-leg soft-tissue defect with the latissimus dorsi free flap.
The flap survived without thrombosis, infection or secondary necrosis. Coverage remained stable, and radiographs confirmed maintained alignment and graft position (Fig. 5). Rehabilitation was initiated with continued outpatient follow-up for union.
Late outcomes and adjunctive wound care. (A) Late postoperative clinical view showing stable healing of soft-tissue coverage with the latissimus dorsi free flap. (B) Late postoperative radiograph demonstrating satisfactory alignment and integration of the pedicled fibular graft within the tibial defect. (C) Adjunctive postoperative wound care with plasma therapy applied to the skin-grafted area over the muscle flap.
Discussion
Gustilo–Anderson type IIIB tibial fractures with segmental bone loss remain limb-threatening because they combine contamination, devitalized tissue, impaired local biology and mechanical instability, which collectively increase infection and non-union risk [3, 6]. Successful limb salvage therefore depends on an integrated strategy: radical debridement, stable fixation, restoration of perfusion, and timely durable soft-tissue coverage [3]. When the bone defect is critical-sized (commonly >6 cm), vascularized bone reconstruction provides living cortical bone with intrinsic blood supply, which may improve union potential and tolerance in contaminated fields compared with non-vascularized grafting [4].
Recipient-vessel status is a key determinant of reconstructive planning. In the present case, computed tomography angiography showed occlusion of the anterior tibial artery and distal peroneal artery, leaving the posterior tibial artery as the sole functional runoff. Under such conditions, performing two independent free transfers (e.g. a free vascularized fibula plus a second free flap for coverage) would increase the microvascular burden on a single vessel and may elevate thrombosis risk. A hybrid approach—a pedicled vascularized fibular graft combined with a single free flap—can reduce the number of arterial anastomoses while still addressing both skeletal and soft-tissue requirements [7].
Using a vascularized pedicled fibular graft from the injured limb offered several practical advantages in this scenario. First, it provided vascularized structural bone to bridge the tibial defect without creating morbidity in the contralateral leg. Second, because the graft remains pedicled, it avoids an additional arterial anastomosis, which is particularly relevant in a single-vessel limb. Vascularized fibular transfer (pedicled or free) is a well-established option for post-traumatic critical tibial defects with high reported union/success rates in appropriately selected cases [8, 9].
For soft-tissue reconstruction of large lower-leg defects, the latissimus dorsi free flap remains a reliable workhorse because it provides substantial vascularized tissue for coverage and infection control, and it can be skin-grafted for definitive closure [5]. In the setting of a single patent artery, an end-to-side arterial anastomosis to the posterior tibial artery allows flap inflow while maintaining distal perfusion; current evidence suggests this technique is a reasonable strategy in traumatic lower-limb reconstruction when preserving flow is critical [10]. Additionally, placing the anastomosis outside the zone of injury is recommended to reduce the risk of vessel spasm or intimal damage and may improve reliability in crush injuries [11]. In our case, these principles enabled stable coverage without thrombosis, infection, or secondary necrosis, facilitating early rehabilitation and maintenance of alignment.
Overall, this case supports the concept that, in complex IIIB tibial injuries with single-vessel runoff, combining a pedicled vascularized fibular graft for skeletal reconstruction with a single free flap for coverage can be an efficient limb-salvage option. This approach minimizes microvascular complexity while providing vascularized bone and soft tissue in one definitive stage, which is particularly valuable when local flap options are limited or unreliable [12, 13].
Conclusion
This case highlights an effective hybrid reconstruction for complex lower-leg defects: a pedicled fibular graft from the injured limb to restore tibial bone loss, combined with a latissimus dorsi free flap for soft-tissue coverage. Limb salvage with functional recovery was achieved with minimal complications, supported by adjunctive VAC CNP 3D Easy-dress and plasma therapy to promote wound healing.
Author contributions
Truong Phu Ho-Man: conceptualization, surgical supervision, manuscript drafting, and final approval. Le Khanh Linh: data collection, literature review, manuscript drafting, and final approval. Tran Van Dung: data collection, critical revision of the manuscript, and final approval.
Conflicts of interest
The authors declare no conflicts of interest.
Funding
No specific funding was received for this work.
Data availability
All data underlying this article are included in the article. Further details are available from the corresponding author on reasonable request.
Ethical approval
Ethical approval was waived for this single anonymized case report according to institutional policy.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}