





Abstract
Hemorrhagic rupture of a simple liver cyst is a rare clinical occurrence. Whether external physical forces can trigger such rupture remains unclear. A 47-year-old woman presented with acute abdominal pain 72 h following an electrical muscle stimulation (EMS) session for weight reduction. Cross-sectional imaging demonstrated a 10-cm ruptured cyst in the right hepatic lobe with associated 1.5 l of hemoperitoneum. Her platelet count was 88 × 109/l. The patient successfully underwent emergency laparoscopic cyst deroofing with povidone-iodine sclerotherapy and did not require blood transfusion. Histopathology confirmed a simple biliary cyst, and a follow-up magnetic resonance imaging at 6 months showed no recurrence. This case suggests that vigorous muscular contractions from EMS may act as a potential precipitating factor for the rupture of large liver cysts, particularly in the context of mild thrombocytopenia, while spontaneous rupture cannot be entirely excluded as an alternative etiology. Laparoscopic management with chemical ablation represents an effective emergency treatment strategy.
Introduction
Simple hepatic cysts (SHCs) are frequently encountered benign liver lesions. Their epidemiology is well-summarized in recent guidelines, including the 2023 EASL clinical practice update [1]. Cyst rupture is an uncommon complication [2]. A review of the literature reveals only 10 reported cases, half of which involved significant hemorrhage [3]. Most events were described as spontaneous, with very few linked to trauma or medical procedures. An unresolved question is whether external mechanical forces—such as those generated during abdominal muscle stimulation—can produce a sufficient pressure differential to cause cyst rupture. This case provides a clinical context to explore this potential mechanism.
Case presentation
A 47-year-old woman was evaluated in the emergency department for acute, severe pain in the right upper quadrant. Three days earlier, she had completed a 30-min session of low-frequency electrical muscle stimulation (EMS) aimed at weight loss, tolerating the procedure without immediate discomfort.
On admission, her vital signs were stable. Physical examination revealed tenderness in the right upper abdomen without guarding or rebound. Laboratory tests showed a platelet count of 88 × 109/l; other parameters were within normal limits.
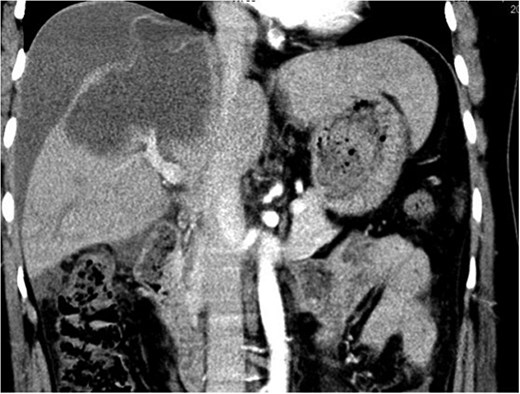
Contrast-enhanced abdominal computed tomography (CT) demonstrated a 10-cm cystic lesion in the right hepatic lobe with a disrupted wall, linear enhancement of the adjacent liver capsule, and a large volume of free intraperitoneal fluid (~1.5 l) (Figs 1 and 2). Diagnostic paracentesis yielded non-clotting bloody fluid.

Contrast-enhanced CT image showing the ruptured right hepatic lobe cyst and surrounding hemoperitoneum.
Contrast-enhanced CT image showing the ruptured right hepatic lobe cyst and surrounding hemoperitoneum.
Emergency laparoscopic exploration confirmed ~1500 ml of hemoperitoneum and an actively bleeding, ruptured cyst on the anterior surface of the right hepatic lobe. Laparoscopic deroofing was performed using an ultrasonic knife, extending to the parenchymal edge. The remaining epithelial lining was then treated with 10% povidone-iodine for chemical ablation. A drain was placed post-procedure. Total operative time was 110 min with an estimated blood loss of <10 ml.
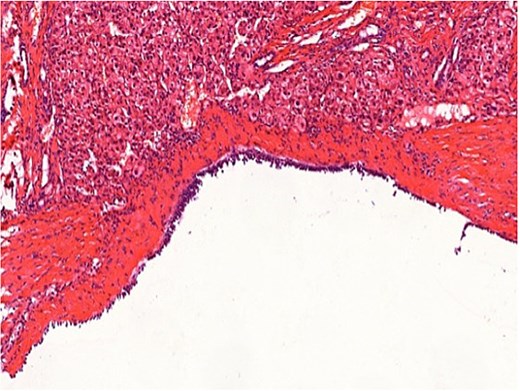
Histopathological examination confirmed a simple biliary cyst with no evidence of parasitic infection or malignancy (Figs 3 and 4). The postoperative course was uneventful, and the patient was discharged on the third day. Follow-up magnetic resonance imaging (MRI) at 6 months showed no recurrence. (Table 1).
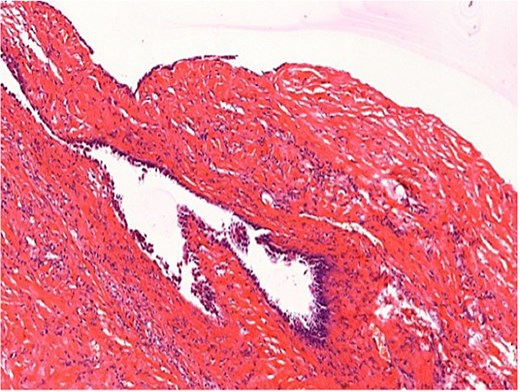
Histopathology (H&E staining, ×200) confirming a simple biliary cyst without features of hydatid disease.
Histopathology (H&E staining, ×200) confirming a simple biliary cyst without features of hydatid disease.
Clinical timeline.
| Time point | Event | Key details |
|---|---|---|
| 3 days pre-rupture | EMS training | The patient did an EMS training session that lasted 30 min. Low-frequency electrical stimulation was used, and the patient had no discomfort during or after the training |
| Day 0, 08:00 | Sudden abdominal pain | The patient felt acute colic in the right upper abdomen, and this pain lasted for 2 h |
| Day 0, 08:30 | Emergency department visit | Vital signs were checked: heart rate was 91 beats per minute, blood pressure was 116/63 mmHg. Tenderness was found when pressing the right upper abdomen |
| Day 0, 09:15 | Imaging test | An abdominal CT scan was done. It showed a 10 cm ruptured cyst in the right liver, along with 1.5 l of ascites in the abdominal cavity |
| Day 0, 10:00 | Diagnostic abdominal paracentesis | 20 ml of non-clotting blood was drawn through paracentesis, confirming internal bleeding in the abdomen |
| Day 0, 11:30 | Surgery started | The surgical plan was laparoscopic cyst unroofing, combined with povidone-iodine chemical ablation for treatment |
| Day 0, 13:20 | Surgery completed | The entire surgery took 110 min. Intraoperative blood loss was less than 10 ml, and the procedure went smoothly without any issues |
| Day 3 post-onset | Discharge from hospital | The patient recovered well after surgery with no complications. A 6-month follow-up MRI scan showed negative results, indicating a successful recovery with no recurrence |
Discussion
Mechanistically, the tonic abdominal contraction induced by EMS can generate a transient increase in intra-abdominal pressure, estimated at 12–15 mmHg based on recent biomechanical models [4]. In the context of a large cyst exceeding 8 cm, Laplace’s law dictates that wall tension is already approaching a critical threshold [5]. The pressure wave from EMS may therefore have acted as a potential precipitating event for rupture, though this causal link remains speculative. To our knowledge, this represents the first reported association between EMS and SHC rupture, and spontaneous rupture cannot be ruled out as the primary cause in this case. Future studies utilizing computational modeling could help quantify the precise pressure dynamics involved and clarify whether a causal relationship exists. The patient presented with a platelet count of 88 × 109/l, which is below the conventional lower limit. Available evidence indicates that
a platelet count below 100 × 109/l is associated with an increased risk of bleeding after hepatic procedures (odds ratio (OR) ~ 2.41) [6, 7]. In patients with large cysts, such thrombocytopenia may impair the hemostatic sealing of minor capsular breaches, thereby potentiating the risk of significant hemoperitoneum upon rupture. While a small randomized controlled trial (RCT) in elective settings demonstrated that povidone-iodine ablation reduces 5-year recurrence from 31% to 8%, no analogous data exist for the emergency management of ruptured cysts [8, 9]. Given the favorable outcome in this case, the adjunctive use of chemical ablation appears clinically reasonable for the emergency management of ruptured SHCs. Establishing a prospective registry to track recurrence and complication rates specifically in ruptured cases would be valuable for developing evidence-based guidelines for this rare clinical scenario. Including the present case, a total of 18 cases of ruptured SLC have been reported in the literature since 1970, and hemorrhage complicated 17 of these cases (94.4%), with 16 requiring surgical intervention [10–17]. While prior cases have been attributed to trauma, spontaneous rupture, or iatrogenic causes [11], this case expands the spectrum of potential triggers by proposing EMS as a plausible contributor rather than a definitive causal factor, and highlights the need for further investigation into the potential association between external abdominal muscle stimulation and hepatic cyst rupture.
Conclusion
EMS may act as a potential precipitating factor for the rupture of large SHCs, particularly in the setting of thrombocytopenia. Laparoscopic deroofing combined with iodine ablation offers a safe and effective emergency treatment. Further studies should aim to identify cyst size and platelet thresholds that might guide preventive measures for patients with large hepatic cysts undergoing external physical interventions.
Conflicts of interest
None declared.
Funding
The fund project information and the corresponding fund number have been submitted in the original manuscript. Relevant details are retained in the editorial submission system of the journal. Medical Research Program of Jiangsu Provincial Health Commission, No. Z2023017;Suqian Science and Technology Program, No. S202317; and Suqian Talent Elite Program, No. SQCG202409.
Patient consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief upon request.

{kind=link}
{kind=link}
{kind=link}
{kind=link}